Purpose
To describe the indications for and approaches to vitreoretinal surgery in patients with osteo-odonto-keratoprosthesis (OOKP).
Design
Retrospective case series.
Methods
This was a retrospective review of all patients who had undergone OOKP surgery between 2003 and 2012 at our center. OOKP procedures were performed for severe ocular surface disease according to the indications and techniques described in the patient demographics of the Rome-Vienna Protocol. Indications for retinal surgery, surgical outcomes, and intraoperative and postoperative complications were documented. Operative techniques were reviewed from the surgical records, and any subsequent surgeries were also recorded.
Results
Thirty-six patients underwent OOKP, and retinal surgery was indicated in 13 (36%). The indications for and approaches to surgery were retinal detachment repair using an Eckardt temporary keratoprosthesis; assessment of retina and optic nerve health prior to OOKP surgery, using either a temporary keratoprosthesis or an endoscope; endoscopic cyclophotocoagulation for intractable glaucoma; endoscopic trimming of a retroprosthetic membrane; or vitrectomy for endophthalmitis with visualization through the OOKP optic using the binocular indirect viewing system. In all cases, retinal surgical aims were achieved with a single procedure. Postoperative vitreous hemorrhage occurred in 16 patients (44%), but all resolved spontaneously.
Conclusions
OOKPs represent the last hope for restoration of vision in severe ocular surface disease, and the retinal surgeon is frequently called upon in the assessment and management of these patients. Temporary keratoprostheses and endoscopic vitrectomies are valuable surgical tools in these challenging cases, improving functional outcomes without compromising OOKP success.
The ocular surface requires a complex system of homeostatic mechanisms to maintain its integrity. Severe cicatricial ocular surface diseases, such as chemical injuries, trachoma and Stevens-Johnson syndrome, destabilize all components of the ocular surface’s protective mechanisms, leading to visual impairment and painful inflamed eyes. Visual rehabilitation in these eyes requires complicated corneal and ocular surface transplantation, but these procedures are rarely successful in eyes with severe end-stage disease.
The osteo-odonto-keratoprosthesis (OOKP) is a procedure in end-stage ocular disease that replaces the cornea with an artificial construct consisting of an optical cylinder embedded in a carrier fashioned from an autologous canine tooth. The procedure has been shown to hold perhaps the greatest promise for the long-term restoration of vision in eyes with the most severe forms of ocular surface disease. In an earlier report from our center, we were able to achieve good vision in 73% of patients with end-stage corneal and ocular surface disorders.
The complexity of OOKP surgery mandates a multispecialty approach involving dental surgeons and ophthalmic surgeons from other subspecialties. In this regard, the vitreoretinal surgeon is frequently involved in the management of patients undergoing OOKP, from the preoperative evaluation of visual potential to the handling of postoperative retinal complications. The vitreoretinal problem associated with OOKP surgery, including retinal detachment (RD), vitreous hemorrhage and endophthalmitis, are potentially blinding, but the management of these complications has not been well described, and the indications, surgical techniques and outcomes for vitreoretinal surgery in the OOKP patient remain poorly defined. In particular, OOKP surgery poses significant challenges in the intraoperative visualization of the posterior segment, and the use of endoscopic vitrectomy and temporary keratoprostheses for visualization during surgery have not been described in detail.
The Singapore OOKP Study has collected data on OOKP implantation in 38 subjects to date. The aim of this study was to describe the vitreoretinal procedures involved in the perioperative management of patients undergoing OOKP, with particular emphasis on the use of the temporary keratoprosthesis.
Methods
This was a retrospective case series of all patients who had undergone OOKP surgery between 2003 and 2012 at the Singapore National Eye Centre. All study subjects were identified from the Singapore OOKP database, a prospective database tracking OOKP procedures performed at our center since 2003. Patient demographics, indications for vitreoretinal surgery, surgical outcomes, and intraoperative and postoperative complications were documented. Operative techniques were reviewed from the surgical records, and any subsequent surgeries were also recorded.
The protocol for the evaluation and management of OOKP patients at our center has been described in detail elsewhere. Briefly, the indication for OOKP surgery is bilateral blindness resulting from end-stage corneal or ocular surface disease not amenable to other corneal or ocular surface transplantation procedures, conforming to the recommendations of the Rome-Vienna Protocol. They include the more extreme forms of Stevens-Johnson syndrome or chemical or thermal burns with severe dry eye and severe destabilization or distortion of the lids, conjunctival fornices and ocular surface complexes. The majority of cases were referred directly by physicians from the Asia-Pacific region, but they also came from Middle East countries and the United States. Specific inclusion criteria included bilaterally blind individuals above the age of 18 years with non-navigable vision (worse than 20/400) in the better eye, but without profound irreversible visual loss from glaucoma, retinal disease, amblyopia, or phthisis bulbi.
OOKP surgery was performed in 2 stages, as described in the Rome-Vienna Protocol. In stage 1, an autologous canine tooth with adjacent mandibular or maxillary bone was removed, and the root was modified to receive an optical polymethyl-methacrylate optical cylinder and then implanted into the cheek beneath the orbicularis oculi. The diseased ocular surface was then fully denuded of corneal and conjunctival epithelium and replaced with a large full-thickness buccal mucosal graft from the inner cheek, extending beyond the rectus insertions. The second stage, performed 2 to 4 months later, involved retrieval of the tooth-cylinder complex for implantation into the cornea through a 5 mm opening. The buccal mucosal flap was first reflected, followed by iris and lens removal and anterior vitrectomy.
The study was performed in accordance with the tenets of the Declaration of Helsinki as revised in 1989. This was an observational, retrospective, noninterventional study and hence did not require Institutional Review Board approval under our institutional guidelines.
Results
A total of 36 patients have undergone OOKP surgery at our center since the start of the program. The most common indication for surgery was severe chemical injury (16 patients; 47%), followed by Stevens-Johnson syndrome/toxic epidermal necrolysis (14 patients; 41%). Other indications included xeroderma pigmentosum, congenital aniridia, severe ocular trauma caused by a grenade, and ocular cicatricial pemphigoid (1 case each). Preoperative visual acuity was defined by hand movements or worse in all cases. The mean duration of follow-up was 2.5 ± 1.9 years. Pre-existing RD was noted in 4 of the 8 patients (50%) who had suffered severe chemical injuries. In these cases, the RD was inferior and peripheral, suggesting anterior traction.
All cases underwent preoperative evaluation by 1 of 3 vitreoretinal specialists (D.W., A.C.L., E.W.). This included A- and B-scan ultrasonography or magnetic resonance imaging (MRI) in selected cases, and electrophysiologic assessment of optic nerve and retinal function. Vitreoretinal surgical procedures were performed for various indications in 13 of the 36 patients (36%) and were employed during stage 1 surgery (pre-OOKP tooth cylinder complex implantation, n = 2); during stage 2 surgery (OOKP tooth cylinder complex implantation, n = 5); or after stage 2 surgery (n = 6) for the management of postoperative retinal complications ( Table ).
| Indication | Type of VR surgery | Number of cases | |
|---|---|---|---|
| Stage 1 OOKP surgery (pre-device implantation) | Repair of RD | TPPV with temporary keratoprostheses | 1 |
| Preoperative assessment of retina and optic nerve status | Endoscopic TPPV | 1 | |
| Stage 2 OOKP surgery (during device implantation) | Repair of RD | TPPV with temporary keratoprostheses during stage II OOKP implantation | 3 |
| Assessment of retina status | TPPV with temporary keratoprostheses during stage II OOKP implantation | 2 | |
| After stage 2 surgery | Management of endophthalmitis | TPPV with temporary keratoprostheses (1); TPPV without temporary keratoprostheses (1) | 2 |
| Trimming of retroprosthetic membrane | Endoscopic TPPV | 2 | |
| Management of glaucoma | Endoscopic cyclophotocoagulation | 1 | |
| Repair of RD | TPPV without temporary keratoprostheses | 1 |
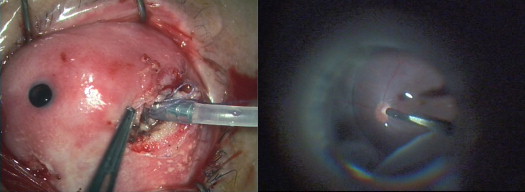
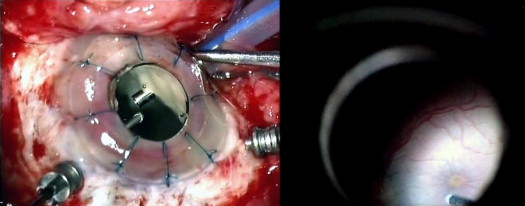
Retinal visualization during surgery was performed through the OOKP optic in 1 case ( Fig. 1 ), using the binocular indirect viewing system (BIOM; Oculus Surgical, Port St. Lucie, FL, USA); endoscopically (Endo-optiks, Little Silver, NJ, USA), using an Eckardt temporary keratoprosthesis that was sutured to sclera after corneal trephination ( Fig. 2 ); or, in 1 case, through a sterilized rigid gas-permeable contact lens temporarily glued over the cornea with cyanoacrylate glue. Endoscopic vitrectomy was performed to assess visual potential in 1 patient. This patient had suffered severe ocular trauma in a grenade attack and had undergone multiple retinal procedures prior to referral to our center. It was thus critical that the retinal status be assessed adequately prior to OOKP surgery, and endoscopic evaluation revealed an inferonasal traction band but no macular scar and a relatively healthy-looking retina otherwise. In this patient, because the history enabled us to determine that the eye was aphakic, we were able to introduce the endoscope directly through the central corneal axis. This avoided the risk for retinal injury caused by a pars plana approach because it was difficult to determine the location of the pars plana due to obliteration of ocular surface’s landmarks. The endoscope was also used to perform endoscopic cyclophotocoagulation (ECP) for glaucoma control in 1 patient and to remove a visually significant retroprosthetic membrane, with the restoration of good visual acuity (20/50) in another. The Eckardt temporary keratoprosthesis was used for RD repair in 1 patient prior to stage I OOKP, and in 3 patients at the time of OOKP stage II implantation, with retinal reattachment achieved in all cases. In a further 2 cases, retinal visualization with the temporary keratoprosthesis at the time of OOKP stage II surgery revealed chronic traction retinal detachments that appeared stable and did not threaten the macula. In 1 patient, infection of the OOKP lamina after stage II implantation complicated by endophthalmitis necessitated the removal of the lamina and vitrectomy using a temporary keratoprosthesis.
Vitrectomy was performed using 20 G vitrectomy instrumentation in all cases that underwent vitrectomy, apart from 1 eye, which underwent sutureless 23 G vitrectomy. We performed sutureless 23 G vitrectomy in 1 patient who had a large hemorrhagic choroidal detachment and retinal detachment after an aborted attempt at stage II OOKP surgery. At the second attempt at stage II implantation, a temporary keratoprosthesis was employed for visualization and 23 G vitrectomy, retinectomy, 360 degree endolaser and silicone oil tamponade were performed, with a good anatomic outcome and a postoperative visual acuity of 20/400.
Postoperative vitreoretinal complications in our series included initial post-OOKP stage 2 vitreous hemorrhage (VH) (16 patients, 44%); retinal detachment (2 patients, 6%); and infectious endophthalmitis (2 patients, 6%). In all cases, the VH resolved spontaneously, and surgery was not required for this indication. Postoperative RD occurred in 2 cases. In 1 of them, redetachment occurred after silicone oil removal. Subsequent endoscopic vitrectomy, retinectomy and reinfusion of silicone oil were successful in achieving reattachment. In the other, a complete RD with closed funnel formation was noted 6 months after OOKP implantation. The vision in this eye was no light perception, and the RD was deemed inoperable. Infectious endophthalmitis occurred in 2 patients, although probably neither case was directly attributable to OOKP implantation. One patient was a carrier of methicillin-resistant Staphylococcus aureus (MRSA) but omitted to inform us of this preoperatively. The other case followed endoscopic transscleral cyclophotocoagulation a full year after successful OOKP surgery and therefore was not a direct consequence of OOKP surgery per se.
The median postoperative visual acuity for the whole cohort was 20/40 (range, 20/20 to no light perception). The best corrected postoperative visual acuity was significantly better in eyes that did not undergo any vitreoretinal procedures (median postoperative visual acuity 20/40 vs 20/120, P = 0.01). OOKP implantation was successful in all cases that underwent vitreoretinal surgery.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


