Vitrectomy for Retinal Detachment
INDICATIONS
The use of vitrectomy for retinal detachment repair is increasing (1) because of a number of factors: more surgeons are trained in vitrectomy, better cutters and fluidics, wide-angle visualization, better methods for drainage of subretinal fluid (SRF) and retinopexy are available, and fellows are less likely to be taught scleral buckling. The decision between vitrectomy, scleral buckling, and pneumatic retinopexy is a very complex issue with few, if any, scientific answers. In general, vitrectomy, gas, and laser should be used when vitreous opacities or tractions make it unlikely that scleral buckling alone will succeed. Relative advantages of scleral buckling include less cataract progression and 80% to 90% success rates in selected detachments. Advantages of vitrectomy include no refractive change; no damage to the extraocular muscles or levator, therefore no strabismus or ptosis; and much less postoperative pain and conjunctival damage. Many surgeons, including the authors, use vitrectomy, gas, and laser in most pseudophakic detachments (2). Many surgeons are inclined to use vitrectomy, gas, and laser for superior detachments and buckling for inferior detachments. Evidence of traction on breaks, especially large horseshoe tears, suggests the need for vitrectomy as does the presence of avulsed vessels. Vitreous blood or significant opacities require vitrectomy to visualize the retinal breaks. The authors rarely use scleral buckling and never combine vitrectomy with scleral buckling. Their current indications for sclera buckling are young phakic patients with clear lenses, retinal detachments with anterior tears, and the absence of proliferative vitreoretinopathy.
SURGICAL SEQUENCE
It is essential to remove as much peripheral vitreous as possible without damaging the lens or creating new retinal breaks. Scleral depression is very useful for this purpose. Wide-angle visualization is essential for peripheral vitreous removal and endolaser and frequently obviates the need for sclera depression vitrectomy. Contact-type wide-angle visualization (Volk or AVI) provides a 10-degree wider field of view than noncontact systems and eliminates all corneal asphericity due to cataract surgery, Limbal Relaxing Incision (LRI), Radial Keratotomy (RK), laser-assisted in situ keratomileusis, Penetrating Keratoplasty (PK), trauma, keratoconus, pterygium, and pterygium removal. In addition, contact-based wide-angle visualization markedly reduces the need for ocular rotation compared to noncontact visualization (BIOM, EIBOS), thereby reducing tool flex with 25- and 27-gauge pars plana vitrectomy.
All traction should be removed from each retinal break. It is crucial to remove traction on the anterior margin as well as from the more apparent flap. Amputation of the flap ensures removal of this component of the traction.
If the breaks or tears can be easily seen after fluid-air exchange, they can be used for internal drainage of SRF. If access to the breaks is difficult, a posterior drainage retinotomy or perfluorocarbon liquids are required. Drainage retinotomy can be initiated by using a disposable bipolar endoilluminator or 25-gauge bipolar diathermy to coagulate, weaken, and mark the site (Fig. 14.1). Outside the arcades, at the most posterior extent of the SRF is often a good location; nasal is better than temporal and superior is better than inferior. Single-cut mode with the vitreous cutter will produce an ideal small, round retinotomy (Fig. 14.2). The soft-tip cannula is preferred for internal drainage of SRF (Fig. 14.3). Internal drainage of SRF should precede fluid-air exchange, especially with the use of preexisting peripheral retinal breaks for drainage; this sequence prevents posterior shift of the SRF. If intraocular lens (IOL) fogging occurs during fluid-air exchange, the air should be removed and perfluorooctane (PFO) used to displace the SRF anteriorly out through the retinal breaks (Fig. 14.4). Endolaser retinopexy is then performed under PFO followed by PFO-gas exchange or medium-term PFO surface tension management. Fogging can be anticipated if a YAG capsulotomy has been performed and the anterior vitreous cortex has been disrupted or removed.
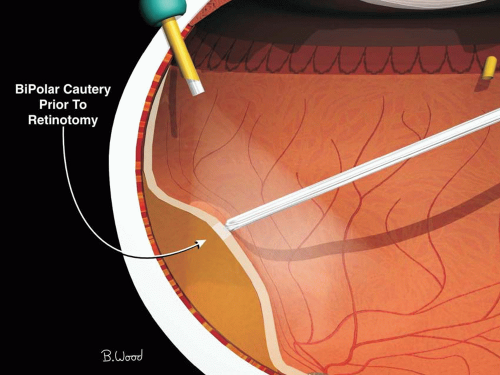 Figure 14.1 ▪ Bipolar diathermy is used to mark the site prior to making drainage retinotomy to facilitate finding the site after retina reattached by internal drainage of SRF and fluid-air exchange. |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


