Purpose
To evaluate the ocular safety of short-term vigabatrin treatment of cocaine abuse.
Design
Multicenter, prospective, randomized, placebo-controlled, double-masked, parallel assignment study.
Methods
Cocaine addicts were randomized to receive vigabatrin 3000 mg/day, cumulative dose 218 g (n = 92), or placebo (n = 94) for 12 weeks. Subjects underwent examination of visual acuity (ETDRS) and peripheral visual field (PVF) by Humphrey Field Analyzer (HFA) 60-4 program before and after treatment. Reliable PVF tests (fixation loss, false positive, and false negative <33%) for 103 subjects were included for the analysis. The threshold visual sensitivity (TVS) was analyzed by points, rings and zones. Main outcome measures included visual acuity decrease by 15 letters and/or significant PVF alteration, defined as 5 or more visual field location points having greater than or equal to 15 dB reduction in TVS or decline (≥33% loss) in posttreatment TVS for 1 or more rings.
Results
Visual acuity decrease was detected in 1 eye of a subject receiving placebo and in none receiving vigabatrin. Posttreatment reduction in TVS more than 15 dB in 5 or more adjacent visual field location points combined with reduction in TVS greater than 33% in 1 or more of the rings was detected in 2 of 54 subjects (3.7%) from the vigabatrin group and in 1 of 49 subjects (2%) from the placebo group ( P = .9, NS). None of the PVF changes were bilateral or concentric.
Conclusions
Short-term use of vigabatrin did not cause a decrease in visual acuity or significant peripheral visual field changes in cocaine abusers.
Vigabatrin, a selective inhibitor of GABA transaminase, is well known to cause visual field defect. American ophthalmologists must become familiar with this drug since it is now being used in our country. Vigabatrin has been used in Europe since the 1980s for the treatment of partial epilepsy with or without secondary generalization that is not satisfactorily controlled by other drugs, as well as for the treatment of infantile spasms. It was approved by the US Food & Drug Administration for the same indications in 2009. Visual field defects are reported as adverse effects of long-term vigabatrin use. This visual field loss is typically detected from 9 months to several years after starting therapy. Gonzalez and associates have demonstrated that patients currently receiving vigabatrin treatment or who previously took vigabatrin for a minimum of 1 year had a 59% and 43% rate of visual field constriction, respectively. A similar pattern has been demonstrated in the other study where vigabatrin treatment (ongoing or in the past) continued for at least 6 months. The authors reported visual field constriction in 40% and 22% of cases, respectively. The degree of visual field restriction may be severe and this may have disabling consequences for the patient. However, most of the patients with perimetry-confirmed defects are asymptomatic. Hence, this undesirable effect can only be reliably detected early by systematic perimetry.
Based on available data, the typical pattern of visual field loss is a concentric constriction of the visual field of both eyes, which is generally more marked nasally than temporally. In the central visual field (within 30 degrees of eccentricity), frequently an annular nasal defect is seen. Central visual acuity is usually not impaired. Available evidence suggests that the peripheral visual field loss is irreversible even after discontinuation of vigabatrin.
Vigabatrin has shown potential as treatment for drug dependence (cocaine and/or methamphetamine) and may not have the same risk of visual field loss. The duration of vigabatrin treatment would not be expected to exceed several months. There are limited data showing that short-term vigabatrin therapy does not lead to detectable visual field defect. The current study is aimed at assessing the safety of 3-month vigabatrin treatment for drug dependency using visual acuity (ETDRS) and peripheral vision measured by the Humphrey Field Analyzer (HFA) 60-4 program.
Material and Methods
Visual acuity was measured (using Early Treatment of Diabetic Retinopathy Study [ETDRS] chart and protocol ) and peripheral visual field was evaluated (using Humphrey Field Analyzer [HFA] 60-4 program) in 186 cocaine addicts enrolled in a phase II clinical trial entitled “Vigabatrin for Treatment of Cocaine Dependence” ( ClinicalTrials.gov identifier NCT00611130 ). The study was approved by the appropriate institutional review boards and was conducted in accordance with the standards of the Declaration of Helsinki at 11 sites in the United States. All participating subjects provided written informed consent. Visual acuity and peripheral visual field assessments were not included in clinical trial endpoints but were considered to be safety measures. Approval from the Institutional Review Board (IRB) of the University of Medicine and Dentistry of New Jersey was obtained for the analysis of all visual safety data.
Subjects of both sexes 18 years of age or older, who had been actively using cocaine, were eligible for enrollment. Major inclusion criteria were as follows: male or female at least 18 years of age; seeking treatment for cocaine dependence; able to be assessed for visual field deficits; have normal visual fields; be in generally good health based on history, physical examination, electrocardiogram, and laboratory findings; other specific criteria related to the nature of cocaine abuse (out of scope of the manuscript).
Major exclusion criteria were as follows: has current dependence on any psychoactive substance other than cocaine; has clinically significant ophthalmologic disease, which would preclude safety monitoring; is undergoing treatment for ocular disease or intends to have any ocular surgery or procedure performed during the time of their participation in the trial (glaucoma, ocular hypertension, current use of eye drops to lower intraocular pressure, known visual field defect, high myopia [greater than −10 diopters], macular disease [eg, age-related macular degeneration, diabetic maculopathy, cystoid macular edema], diabetic retinopathy worse than mild background disease, retinal disorder that could affect visual field [eg, prior retinal detachment, retinitis pigmentosa], cataract causing visual acuity less than 20/100, uncontrolled systemic hypertension, abnormality grading of 3 [moderate] or 4 [severe] for ophthalmoscopy or biomicroscopy); have any serious medical or psychiatric illness and/or clinically significant abnormal laboratory value that in the judgment of the principal investigator would make study participation unsafe, or that would make treatment compliance difficult; has ever taken vigabatrin in the past; has received a drug with known major organ toxicity, including retinotoxicity within 30 days of randomization; other specific criteria related to the nature of cocaine abuse (out of scope of the manuscript).
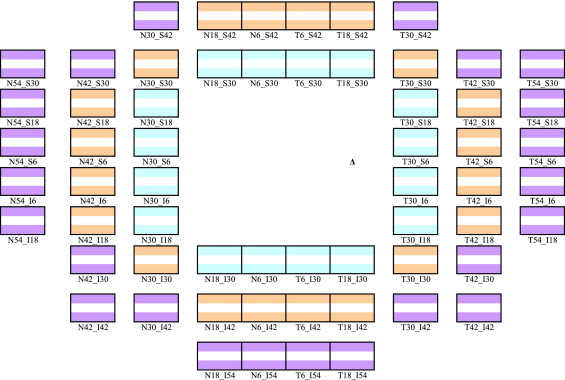
A summary of demographic parameters is presented in Table 1 . Subjects underwent a complete ophthalmic evaluation by an ophthalmologist at baseline. This included an evaluation of best-corrected visual acuity (using the ETDRS visual acuity charts) and slit-lamp and dilated fundus examinations. The visual field testing protocol specified that 2 fields for each eye be taken at the baseline visit: 1 training and 1 baseline test. The visual field test was considered reliable if fixation loss as well as incidence of false-positive and false-negative responses was below 33%. Unreliable visual fields (>33.33% fixation losses, false negatives, or false positives) could be repeated once on the same day or a subsequent day. If a subject was unable to perform reliable visual fields at baseline, then this subject was deemed ineligible for the study. Eligible subjects were randomized into 2 groups: vigabatrin group (n = 92) and placebo group (n = 94). Subjects of both groups underwent visual acuity and visual field testing before and after treatment. If a follow-up visual field test was deemed unreliable it was repeated within 14 days. The duration of treatment in both groups was 12 weeks. Subjects received vigabatrin or placebo matching the vigabatrin tablets in size and appearance. The vigabatrin dose was escalated over a 2-week period up to 3000 mg/day, maintained at this dose for 9 weeks, and tapered to 0 during week 12. The total dose of vigabatrin reached 218 g. The threshold visual sensitivity (TVS) was analyzed by points and rings as previously described. Three rings were used for the analysis of TVS: inner ring (16 location points), middle ring (20 location points), and outer ring (24 location points) ( Figure 1 ) . Total TVS (sum of sensitivity throughout all location points/rings) was also calculated. Visual field change was defined significant per protocol, in part based on the pilot study, if one of the following occurred: 1) 5 or more adjacent visual field location points had greater or equal to 15 dB reduction in TVS; 2) reduction in TVS ≥33% occurred in 1 or more rings. The Student t test was used to compare continuous variables. χ 2 or Fisher exact test was used to examine the difference in proportions between groups. The P value ≤ .05 was considered a statistically significant difference.
| Parameter | N (%) or Range (Mean ± SD) | P Value | |
|---|---|---|---|
| Placebo (n = 94) | Vigabatrin (n = 92) | ||
| Race | |||
| Black or African-American | 52 (55.3%) | 60 (65.2%) | .17 |
| White | 31 (33%) | 27 (29.3%) | .59 |
| Native American | 2 (2.1%) | 0 (0%) | .25 |
| Other | 9 (9.6%) | 5 (5.4%) | .28 |
| Sex | |||
| Male | 64 (68%) | 60 (65%) | .68 |
| Female | 30 (32%) | 32 (35%) | |
| Age (years) | 21–61 (45.0 ± 8.3) | 23–69 (44.6 ± 7.6) | .51 |
| Cocaine use self-reported (days during last 30 days before screening) | |||
| 18 days or less | 62 (66%) | 64 (69.5%) | .59 |
| More than 18 days | 32 (34%) | 28 (30.5%) | |
| Primary method of cocaine administration | |||
| Smoking/intravenous | 81 (86%) | 78 (85%) | .79 |
| Snorting | 13 (14%) | 14 (15%) | |
Results
Demographic parameters were not statistically different between the vigabatrin and control groups. Ophthalmic evaluation by an ophthalmologist on completion of the study did not reveal any detectable acquired abnormalities in any subjects. There was no change in best-corrected visual acuity detected after 12 weeks of treatment within the vigabatrin group, while a reduction in visual acuity by 15 letters was detected in 1 eye of 1 of the subjects within the placebo group. Pretreatment and posttreatment reliable peripheral visual field tests from 103 subjects who completed the medication treatment phase were included in analysis. In both placebo and vigabatrin groups, there were no statistically significant differences between baseline and posttreatment mean total TVS ( Table 2 ). Statistically significant difference in mean TVS before and after treatment was found only in the middle ring in the vigabatrin group. The values of mean total TVS as well as mean ring TVS at compared time points did not significantly differ between placebo and vigabatrin group. Mean total TVS as well as mean ring TVS in subjects judged compliant with vigabatrin treatment regimen did not differ from subjects on placebo treatment ( Table 2 ). Posttreatment reduction in TVS more than 15 dB in 5 or more visual field location points combined with reduction in TVS greater than 33% in 1 or more of the rings was detected in 2 of 54 subjects (3.7%) from the vigabatrin group ( Figure 2 , Top and Middle) as well as in 1 of 49 subjects (2%) from the placebo group ( Figure 2 , Bottom) ( P > .05, NS). Visual fields from these subjects were evaluated to identify whether any had characteristic changes associated with vigabatrin. None did. Bilateral concentric visual field alterations were not revealed in any of these subjects with significant change identified per protocol. Additionally, all visual fields of subjects exposed to vigabatrin were evaluated regardless of whether they reached a predefined endpoint. None of the subjects exposed to vigabatrin demonstrated characteristic visual field changes.
| Mean Total TVS | Mean Inner Ring TVS (30 Degrees From Fixation) | Mean Middle Ring TVS (30 to 42 Degrees From Fixation) | Mean Outer Ring TVS (42 to 54 Degrees From Fixation) | |
|---|---|---|---|---|
| Placebo treatment (n = 49) | ||||
| Before treatment | 2338 ± 392 | 782 ± 105 | 814 ± 137 | 741 ± 167 |
| After treatment | 2350 ± 381 | 792 ± 93 | 824 ± 131 | 734 ± 179 |
| Vigabatrin treatment (n = 54) | ||||
| Before treatment | 2385 ± 351 | 791 ± 86 | 839 ± 126 | 755 ± 154 |
| After treatment | 2289 ± 463 | 769 ± 119 | 797 ± 162 b | 723 ± 193 |
| Compliant with vigabatrin treatment (n = 17) | ||||
| Before treatment | 2449 ± 339 | 801 ± 82 | 861 ± 139 | 787 ± 182 |
| After treatment | 2363 ± 498 | 779 ± 116 | 818 ± 168 | 766 ± 221 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


