Purpose
To identify clinical, demographic, immunologic, and health-related quality-of-life data from a cohort of vernal keratoconjunctivitis (VKC) patients with the onset of the disease after puberty (VKC-like disease).
Design
Retrospective, observational case series.
Methods
Forty-nine patients with late-onset VKC-like disease from among 600 consecutive VKC patients. History of disease, test results for allergen sensitivity, signs and symptoms, impact of disease on work productivity, health-related quality of life, and treatment satisfaction were assessed. In addition, multiplex bead analysis for Th1/Th2 cytokines were carried out in tear samples from 20 VKC patients (10 adults and 10 children) and from 10 normal subjects.
Results
A family history of allergy was positive in only 28% and positive prick test results were present in 55% of the 49 VKC-like adult patients. Based on typical signs and symptoms, 48% were affected by the limbal form, 33% were affected by the tarsal form, and 19% were affected by the mixed form. Corneal ulcer complicated the disease in only 2 adult patients. Although the disease was not considered a limiting factor for work, productivity was reduced by 26% and social activities were reduced by 31% during active flare-ups. No significant differences were found in tear cytokine pattern production between VKC in children and VKC in adults.
Conclusions
A late onset VKC-like disease can appear in young adults with signs and symptoms similar to those in pediatric disease, but with less corneal involvement.
Vernal keratoconjunctivitis (VKC) is a chronic, bilateral inflammation of the conjunctiva that generally affects children and young adults who have an atopic personal or family history and live in warm climates. Although the allergic nature of this disease is widely accepted, in less than 50% of cases, it is associated with other allergic manifestations and specific immunoglobulin E (IgE) sensitization. The predilection for males and the resolution after puberty suggest a role of hormones in the development of VKC; however, the exact mechanisms behind this association are still unknown.
Although it is considered a long-term disease with an average duration of 4 to 8 years, VKC generally subsides before or just after puberty. It can persist or reactivate after puberty; however, a VKC-like disease has been found in young adults without any history of allergic disease in childhood. This new clinical entity is characterized by signs and symptoms similar to the typical VKC. Studies of large cohorts of subjects revealed that VKC is present between 3% to 10% of school-age children in endemic areas such as Cameroon, Turkey, and Israel. In Morocco, India, and Senegal, it accounts for 6% of new ophthalmic referrals and up to 90% of new ophthalmic referrals in persons younger than 15 years. A survey of ophthalmologists from 6 European countries has identified a prevalence rate of 3.2 per 10 000 inhabitants in Western Europe. In Italy alone, the incidence of VKC was calculated to be 7 per 100 000 subjects younger than 16 years and 0.06 per 100 000 subjects older than 16 years, with a greater incidence in males only in the pediatric patients. In most of these published retrospective case series, little is known about the exact age of the described young adults in whom the disease developed after puberty. Although the management of VKC in young patients is challenging, adult patients may have a lower compliance to self-administered treatments and higher complication rates.
The aim of the present study was to assess clinical, demographic, immunologic, and health-related quality-of-life data from a cohort of patients with a VKC-like disease that presented after puberty. Additionally, in a subgroup of these patients, multiple cytokines were defined in tears during the inflammatory phase of the disease to identify any potential differences in cytokine patterns between adults and children.
Methods
Patients
A diagnosis of VKC was based on the patient’s history and the presence of typical clinical signs and symptoms. The disease was classified as: tarsal (by the presence of giant papillae more than 1 mm in diameter), limbal (by the presence of limbal infiltrates and Trantas dots), or mixed (by the presence of both limbal and tarsal signs). The database, created using the Access software program (Microsoft Corporation, Redmond, Washington, USA), included 600 consecutive VKC patients referred to the Ocular Allergy Service of the Ophthalmology Department at the University of Padua from 1996 through December 2011. This retrospective observational case series study complied with the tenets of the Declaration of Helsinki and was approved by the Padova University Hospital Review Board. The following information was collected: family and personal medical history, age at onset and resolution of the disease, associated allergic manifestations, results of skin prick test for allergen sensitivity, serum specific IgE to a panel of 24 allergens (FEIA, CAP System; Pharmacia, Uppsala, Sweden), total serum IgE (UNICAP; Pharmacia), serum levels of eosinophil cationic protein (UNICAP), treatment history, and outcome. The patients’ written informed consent to obtain blood samples and to analyze clinical and demographic data was confirmed on record.
To define the adult onset of VKC, a fixed cutoff age of 15 years was chosen, with the assumption that at this age, most patients already had attained puberty. Patients with a diagnosis of VKC in childhood and recurrence of signs and symptoms after puberty were excluded (11 of 600). The presence or history of eczema was an exclusion criterion. Clinical findings of a complete ophthalmic examination, performed at least once yearly, were recorded. An overall clinical score for disease severity, considering immediate signs and symptoms as well as permanent changes (i.e., papillae size or corneal scars), was defined as follows: 0 = quiescence or absence of symptoms; 1 = mild seasonal signs and symptoms without corneal involvement, 2 = mild persistent signs and uncomfortable seasonal symptoms without corneal involvement, 3 = severe intermittent signs and uncomfortable persistent symptoms with mild corneal involvement, and 4 = very severe persistent signs and symptoms with diffuse superficial keratopathy or ulcer graded by a standardized clinical grading system. Single signs and symptoms also were graded using a predefined 0-to-4 scale.
Tear samples were collected from the outer canthus with a microcapillary tube, and the percentages of eosinophils, neutrophils, and lymphocytes present in 5 microscopic fields were counted on precolored slides (Testsimplets; Waldeck GmbH & Co, Münster, Germany) using a Zeiss microscope (Carl Zeiss Microscopy GmbH, Jena, Germany) at ×312 magnification.
The impact of the disease on work or study productivity, on social life, and on treatment satisfaction was evaluated using a visual analog scale (in which 0 indicated no symptoms and 100 indicated the worst symptoms ever experienced).
A modified version of the Quality of Life in Children with Vernal Keratoconjunctivitis (QUICK) questionnaire was completed by the adult VKC-like patients ( Table 1 ), all of whom were recalled and were examined during their active phase. The original final version of the QUICK questionnaire was designed specifically to be completed easily and quickly by 5- to 12-year-old children with chronic keratoconjunctivitis. For the purpose of the present study in adult patients, items regarding school or play activities were deleted and answers were graded with a 0-to-4 scale scoring system similar to that of signs and symptoms (0 = absence; 4 = very severe/persistent all the time).
| In the Last Month, Because of Your Conjunctivitis, Did You: |
|---|
| Feel burning in your eyes? |
| Have trouble staying in air-conditioned rooms? |
| Have itchy eyes? |
| Have to use tissues? |
| Have eye secretion? |
| Have puffy eyes? |
| Have red eyes? |
| Have problems in the light? |
| Have tearing? |
| Have eye secretion? |
| Have closed and sticky eyes in the morning? |
| Have blurred vision? |
| Have to use eye drops? |
| Have difficulties concentrating at work or other activities? |
| Have difficulties in reading? |
| Have trouble meeting your friends? |
| Have trouble practicing sports? |
| Have trouble going to the pool? |
Tear Cytokines
Tear samples were collected with a capillary tube from a subgroup of 10 adult active VKC-like patients (5 affected by the tarsal form and 5 by the limbal form), from 10 children affected by active VKC (5 affected by the tarsal for and 5 limbal VKC), and from 10 normal subjects. Samples were diluted 1:1 and were analyzed using multiplex bead analysis, which uses microspheres as a solid support for immunoassays and allows for analyses of all molecules in each sample. Th1-type (interleukin [IL]-2, IL-12, interferon-γ), Th2-type (IL-4, IL-10, and granulocyte-macrophage cell stem factor), and proinflammatory cytokines (IL-1β, IL-6, IL-8, and tumor necrosis factor-α) were measured according to the manufacturer’s instructions (Upstate Biotechnology UK, Buckingham, UK). Briefly, samples were incubated with antibody-coated capture beads for 2 hours at 20 C. Washed beads were incubated further with biotin-labeled antihuman cytokine antibodies for 1 hour followed by streptavidin-phycoerythrin for 30 minutes. Samples were analyzed using a Luminex 100 (Luminex, Austin, Texas, USA) with Starstation software (Applied Cytometry Systems, Sheffield, UK). Standard curves of known concentrations of recombinant human cytokines were used to convert fluorescence units to cytokine concentration (picograms per milliliter). Minimum detection levels for each cytokine were as follows: 20 pg/mL (IL-2), 10 pg/mL (IL-1βIL-8, IL-12, tumor necrosis factor-α, 5 pg/mL (IL-4, interferon-γ), 2 pg/mL (IL-10), and 1 pg/mL (IL-6).
Statistical Analysis
Differences between percentages were compared using the chi-square test. Differences between mean values were compared using the Student t test. The cytokine data sets were analyzed for normal distribution using the Kolmogorov-Smirnov normality test. Because most of the data sets were not normally distributed, the nonparametric Kruskal-Wallis analysis with the Dunn multiple comparison posttest was used. The minimal level of confidence at which the results were judged significant was P < .05. Data are reported as mean ± standard deviation.
Results
Of the 600 VKC patients classified in our database from 1996 through December 2011, 49 demonstrated a VKC-like disease after 15 year of age. Of these, 32 (65.3%) were male and 17 (34.7%) female, with a male-to-female ratio of 2:1, which was statistically significant less than the male-to-female ratio found in our pediatric VKC population ( Table 2 ). In the VKC-like patients, the mean age of disease onset was 20 ± 4 years, with no significant difference between males and females or clinical form of the disease. The disease resolved completely in only 9 patients. In this subgroup, the mean length of the disease was 6.4 ± 4.8 years, with 1 case lasting 13 years. All patients were recalled and examined at least once yearly and at the time of this retrospective study.
| Male-to-Female Ratio | Tarsal Form (%) | Limbal Form (%) | Mixed Form (%) | Positive Family History for Allergy (%) | Corneal Ulcer (%) | Asthma (%) | Rhinitis (%) | Skin Diseases (%) | Total Serum IgE (KU/L) | Eosinophil Cationic Protein (μg/L) | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Adults | 2:1 | 45 | 33 | 19 | 28.6 | 4.2 | 10 | 22 | 12 | 154 ± 281 | 29 ± 19 |
| Children | 4:1 | 28 | 57 | 15 | 42.8 | 18.2 | 12 | 26 | 16 | 469 ± 1214 | 34 ± 32 |
| P value | .049 | NS | NS | NS | .06 | .011 | NS | NS | NS | .01 | NS |
All VKC-like patients had a clinical history of conjunctivitis with annual recurrences between March and October, with symptoms characterized by itching, burning and discharge, onset after puberty, and no history of VKC, seasonal allergic conjunctivitis, or atopic dermatitis in childhood. The skin of the lid and lid margin was not involved in all of these patients. Based on the overall severity score, during the season, 75% of the patients were considered to have a grade 2 or 3 of the disease. Tear cytologic analysis showed the presence of eosinophils in all VKC-like patients during their active inflammatory phase, with a percentage of eosinophils between 5% and 45% of the inflammatory cells in tears.
A significant association with ovarian cysts unaccompanied by hyperandrogenism was reported in the female population (50%).
Clinical Forms
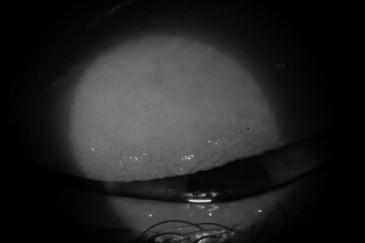
The tarsal form of the disease in adult patients appeared either as a diffuse thickness of the upper tarsal conjunctiva with a diffuse subepithelial fibrosis without giant papillae or with formation of the typical giant papillae of variable size and shape ( Figure 1 ). The limbal form was characterized by the presence of transient grayish, gelatinous-like or yellow-white nodules at the limbus associated with conjunctival hyperemia more pronounced in the limbal and in the perilimbal area ( Figure 2 ). Family history for allergy, distribution of clinical forms, and incidence of corneal ulcers in adult and children VKC patients is shown in Table 2 , as well as associated allergic manifestations and allergy serum biomarkers results. No significant permanent reduction of best-corrected visual acuity or keratoconus was reported in the VKC-like group of patients.
Allergy Diagnostic Tests
A positive skin prick test was identified for at least 1 allergen in 55% of adult VKC-like patients (27 of 49 patients) and in 43.2% of VKC children. In the adult group, the results of the test identified a sensitization to Dermatophagoides in 40.4%, to Graminaceae in 39%, to Parietariae in 13.7%, and to food allergens in 2.6%, with no significant differences compared with the distribution of specific sensitizations in children. The limbal form in adults was associated more frequently with positive prick test results (65.2%) compared with children (37.1%). This difference was statistically significant ( P = .0093).
Specific serum IgE tests demonstrated positive results for at least 1 allergen in 57% of the adult patients (28/49 patients) and in 51% of children. In the adult group, the results of specific serum IgE were associated with the results of prick tests in 70% of the cases and identified a positive sensitization to Graminaceae in 28% of patients, to Dermatophagoides in 36% of patients, to Alternaria in 11% of patients, to tree pollens in 10% of patients, to Parietariae in 14% of patients, to Compositae in 3% of patients, and to food allergens in 3.7% of patients. Levels of total IgE were significantly higher in prick test-positive and specific IgE-positive patients (271 ± 390 KU/L) compared with patients with negative results (59 ± 66 KU/L; P < .05). Similar results also were found in VKC children (positive prick test results, 849 ± 1761 KU/L; negative prick test results, 140 ± 193 KU/L; P < .0001).
Quality-of-Life Test in Adult Vernal Keratoconjunctivitis Patients
The mean duration of symptoms was 6.21 ± 2.5 months/year (range, 3 to 12 months/year), especially between April and September. The most common nonspecific trigger factor was environmental exposure to sun and dust (scores of 3 to 4 in 50% of patients; Figure 3 ). Only 31% of patients indicated pollen exposure as a severe (score 4) triggering factor.



