Purpose
To determine the clinical utility of intraocular videoendoscopy examination for the evaluation of the retina and optic nerve in patients being considered for a Boston type I keratoprosthesis (KPro).
Design
Interventional case series study.
Methods
Ten patients with a history of corneal blindness caused by failed penetrating keratoplasty (PK) and inability to accurately assess visual potential were included in this study. Ophthalmologic examination, B-scan ultrasonography, and pars plana videoendoscopy were carried out to assess the retina and optic nerve before KPro.
Results
Posterior segment examination was successfully used to evaluate the retina and optic nerve of all patients with opaque corneas. Out of 10 patients that underwent endoscopic examination, 3 (30%) were considered to be adequate candidates for KPro surgery and 7 (70%) were not. This was based on visualized retinal disease and/or optic nerve pathology. Of the 3 patients that underwent KPro surgery, all of them had a significant improvement of vision, including counting fingers to 20/100, hand motion to 20/5, and light perception to 20/80, as suggested by the endoscopy preoperative examination. No complications of the endoscopy procedure were observed.
Conclusions
This report demonstrates the successful use of intraocular videoendoscopy to rule out threats to a good visual outcome for patients being considered as candidates for KPro. Direct visualization of the posterior segment can be part of the preoperative algorithm in the decision process of performing a KPro surgery in patients when visual potential is questionable.
Endoscopy, derived from the Greek words endon (“within”) and skopein (“to view”), has been widely used for the diagnosis and treatment of disease. The first prototype of an ocular endoscope was reported in 1934 by Thorpe, for removing nonmagnetic intravitreal foreign bodies. Since then, significant technological advances in microsurgical instrumentation have led to the increased use of endoscopy in ophthalmic surgery. The use of the endoscope in ophthalmology has been mostly used in vitreoretinal surgery. More recently, this technique has proven to be a useful alternative in anterior segment surgery and glaucoma, usually when the image is limited by poor ocular media, such as the presence of corneal opacity.
Corneal disease, characterized by scarring and opacification, constitutes the second most common cause of blindness. After using 1 or more corneal grafts that may fail in these patients, the use of Boston type 1 keratoprosthesis (KPro) has become the next option of therapy for visual rehabilitation. Although published data have demonstrated the successful use of the KPro in the treatment of corneal blindness, the postoperative care of these patients is complex and is associated with significant complications. Bradley and associates recently reported that even though the Boston type 1 KPro is a viable option after multiple keratoplasty failures, there is a significant number of complications associated with this procedure, including glaucoma, retroprosthetic membranes, vitritis, and endophthalmitis. Therefore, patient selection is crucial in the decision process during the preoperative assessment of these patients to assure that only patients that will ultimately benefit are considered for KPro surgery.
Nevertheless, the determination of vision potential can be difficult in patients with an opaque cornea. Potential acuity meter, laser interferometry, and other techniques usually used in determining potential vision are not very useful in patients with advanced ocular surface disease. In most instances, function is determined by light perception examination and anatomic normality is determined with ultrasound examination; however, this approach has major limitations. In fact, even patients with normal ultrasonography and counting fingers vision may have significant optic nerve or macular pathology that would limit their vision potential. Direct visualization of the posterior segment in these patients could be a major determining factor in the final decision of whether to proceed with surgery.
The objective of this study was to determine if the use of intraocular videoendoscopic direct examination of the posterior segment of KPro candidates with questionable vision potential could be safely used to predict a good visual outcome after KPro surgery. With this study, we aimed to gain a tool to help us in the preoperative decision process to determine if the placement of a KPro would benefit a certain patient.
Our data demonstrate that the clinical utility of the intraocular videoendoscopy for the evaluation of the retina and optic nerve prior to the placement of a Boston type 1 KPro is safe and relatively easy to perform. Moreover, the clinical findings obtained by visualization of the posterior segment with intraocular videoendoscopy accurately predicted a good surgical outcome in patients in whom the endoscopic examination was found to be within normal limits. Therefore, intraocular videoendoscopic examination can be a major determining factor in the decision process to perform or to defer KPro surgery in selected patients.
Methods
This study consisted of an interventional case series of consecutive patients that underwent a diagnostic endoscopic procedure at the Bascom Palmer Eye Institute, Department of Ophthalmology, University of Miami Miller School of Medicine and the Centro Oftalmologico de Valencia during the period April 2011-April 2012. The study was completed December 2012. The protocol was approved by the Institutional Review Board (Medical Science IRB A University of Miami, No: 20090935; January 21, 2010). Patient data were collected and maintained in accordance with Health Insurance Portability and Accountability Act guidelines. An Institutional Review Board–approved and Health Insurance Portability and Accountability Act–compliant clinical protocol and surgical consent form for endoscopic procedure were developed and enrollment was initiated for patients with blindness caused by corneal opacity. All patients or their legal representatives signed an informed consent form.
The indication for endoscopic examination was questionable hand motion (HM) to light perception (LP) vision in patients with corneal blindness resulting from severe corneal opacity and vascularization caused mainly by corneal ulcers, ocular trauma, trachoma, or anterior segment dysgenesis. All patients had a history of multiple corneal surgeries, corneal grafts, or ocular surface transplantation procedures and were deemed high risks for standard keratoplasty. The better or only eye had poor vision, such as LP, HM, or, at best, counting fingers (CF).
Data from each patient were recorded on the basis of a detailed ocular history and examination. Previous ophthalmologic records were reviewed to identify the reasons for failure of corneal graft or other surgeries. The data collected included age, sex, ocular history, medical history, eye affected, preoperative best-corrected visual acuity, anterior segment examination findings on the slit-lamp biomicroscopy, and posterior segment examination findings by B-scan ultrasonography and videoendoscopy. The major determinants of whether to perform or withhold KPro surgery were anatomic findings (eg, status of retina and optic nerve after intraocular videoendoscopic evaluation).
Surgical Technique
All the procedures were performed by 3 surgeons (T.A.A., A.M.B., and J.M.V.), using peribulbar anesthesia under monitored anesthesia care. The endoscopic system used was an E-4 Microprobe, manufactured by Endo-Optiks (Little Silver, New Jersey, USA) ( Figure 1 ).
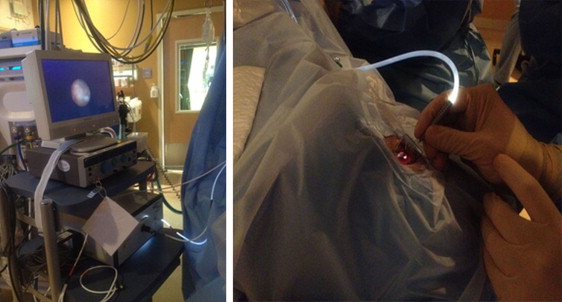
A 23 gauge infusion line was placed inferotemporally. A small, localized peritomy was created superotemporally and a 20 gauge sclerotomy was created 4 mm posterior to the surgical limbus at that location. The endoscopy probe was checked prior to placing it in the eye and a clinically adequate image was obtained with the probe prior to its insertion into the eye ( Figure 1 ). First, the infusion was checked for correct position through the choroid and in the vitreous cavity, under direct observation with the endoscopy probe, the infusion was started. Next, the endoscopy probe was used to perform a systematic examination of the peripheral retina and posterior pole. After the examination, the endoscopy probe was removed from the eye, the sclerotomy was closed with a 7-0 vicryl suture, the overlying conjunctival defect was repaired, the infusion line was removed, and the sclerotomy was closed with 7-0 vicryl suture.
Results
A total of 10 eyes underwent intraocular videoendoscopic evaluation. The age ranged from 14 to 89 years (median, 47.6 years) ( Table 1 ). Five patients were male and 5 were female. The most common cause of corneal blindness was previous corneal ulcer (3 eyes), anterior segment dysgenesis (2 eyes), and ocular trauma (2 eyes). Of the 10 eyes that underwent endoscopic evaluation, 1 had a history of 3 penetrating keratoplasties (PK), 5 had a history of 2 prior corneal transplantations, 2 were cases of retinal detachment with silicone oil and intraocular lens extraction, 4 cases had previous cataract surgery, and 1 case had glaucoma surgery with a glaucoma drainage implant. All patients had media opacities characterized by the presence of an edematous, vascularized, and opacified corneal graft.
| Case | Age (y) | Sex | Eye | Etiology of Cornea Blindness | Previous Surgeries | Anterior Segment Findings |
|---|---|---|---|---|---|---|
| 1 | 14 | M | OD | Sclerocornea | PK, PPV, glaucoma tube shunt | Edematous, vascularized, opacified cornea graft |
| 2 | 22 | F | OS | Aniridia | 2 PK | Edematous, vascularized, opacified cornea graft |
| 3 | 85 | F | OS | Trachoma | 3 PK, cataract surgery | Edematous, vascularized, opacified cornea graft |
| 4 | 89 | F | OD | Failed PK | RD surgery with silicone oil, IOL extraction, PK | Edematous, vascularized, opacified cornea graft; sectoral iris atrophy |
| 5 | 41 | F | OD | Ocular Trauma | PK, cataract surgery | Edematous, opacified cornea graft, calcium deposits |
| 6 | 52 | M | OD | Corneal ulcer | 2 PK, cataract surgery | Edematous, vascularized, opacified cornea graft |
| 7 | 50 | M | OD | Corneal ulcer | 2 PK, cataract surgery | Edematous, vascularized, opacified cornea graft |
| 8 | 14 | M | OD | Corneal ulcer | 2 PK | Edematous, vascularized, opacified cornea graft. |
| 9 | 45 | F | OS | Failed PK | 2 RD surgery with silicone oil, PK | Edematous, vascularized, opacified cornea graft |
| 10 | 64 | M | OS | Chemical burn | ALT, 2 PK | Edematous, vascularized, opacified cornea graft |
The preoperative visual acuity varied between LP (4), HM (4), CF (1), and no light perception (1); B-scan ultrasonography was performed in all 10 patients. Three eyes presented with vitreous opacity, 1 case had diffuse choroidal thickening, another case had changes suggestive of macular edema, 1 eye had a slightly elevated optic disc, and another had silicone oil in the vitreous cavity.
Using videoendoscopy technique, we identified 4 eyes with optic nerve damage ( Figure 2 ); 4 with retinal detachments, 2 with proliferative vitreoretinopathy (PVR), another 3 had maculopathy, and 1 had a retinal hemorrhage. Please note that some eyes had more than one finding in the endoscopic exam.
According to these findings, 3 of 10 patients (30%) were considered to be good candidates for KPro surgery and 7 (70%) were not ( Table 2 ). Of the 3 patients that underwent KPro surgery, all of them (3/3) had a significant improvement of vision (CF to 20/100, HM to 20/50, LP to 20/80) ( Figure 3 ). These results confirmed the normal findings observed by the endoscopy preoperative examination. Importantly, none of the patients in our series had a detrimental change of their baseline preoperative visual acuity and no complications of the endoscopy procedure were observed.
| Case | Eye | Preoperative Vision | USG Findings | Video Findings | Postoperative Vision | Decision Based on Endoscopy |
|---|---|---|---|---|---|---|
| 1 | OD | LP | Vitreous opacities with vitreous membrane, optic disc elevation, no retinal or choroidal detachment, irregular and sloped globe | Significant maculopathy with RPE atrophy, optic nerve pallor, tractional membranes | LP | No KPro surgery |
| 2 | OS | HM | Diffusely choroidal thickened with probable choroidal detachment Probable shallow temporal posterior retinal detachment | Chronic retinal detachment, PVR, preretinal hemorrhage | HM | No KPro surgery |
| 3 | OS | CF | Vitreous opacities with a posterior vitreous detachment, macular thickening, posterior staphyloma | Disc and macula appeared healthy (there is only sign of myopic degeneration) | 20/100 | KPro surgery |
| 4 | OD | HM | Siliconized eye, no RD but it is not meaningful | Chronic retinal detachment, PVR | HM | No KPro surgery |
| 5 | OD | LP | Pseudophakic, applied retina, PVD | Slight pallor optic nerve, macular hole, PVD | HM | No KPro surgery |
| 6 | OD | LP | Aphakia, PVD, applied retina | Chronic retinal detachment, PVR | HM | No KPro Surgery |
| 7 | OD | HM | Aphakia, vitreous opacity, applied retina | Disc and macula appeared healthy | 20/50 | KPro surgery |
| 8 | OD | LP | Applied retina | Disc and macula appeared healthy | 20/80 | KPro surgery |
| 9 | OS | HM | Aphakia, macular edema, retinal detachment | Optic nerve pallor, macular hole, chronic retinal detachment | LP | No KPro surgery |
| 10 | OS | NLP | Mild vitreous opacities, no RD, no mass lesion, no obvious cupping | Optic atrophy | NLP | No KPro surgery |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


