and Mitrofanis Pavlidis2
(1)
Department of Ophthalmology, Uppsala University Hospital, Uppsala, Sweden
(2)
Augencentrum Köln, Cologne, Germany
Electronic supplementary material
The online version of this chapter (doi:10.1007/978-3-319-20236-5_3) contains supplementary material, which is available to authorized users.
Electronic supplementary material
for this chapter is accessible online at http://extras.springer.com/ by searching via the ISBN.
All 27G instruments allow to operate more delicate and atraumatic than 25G or 23G instruments. This results in less trauma and faster postoperative recovery.
3.1 Insertion of Trocars (Figs. 3.1, 3.2 and 3.3)
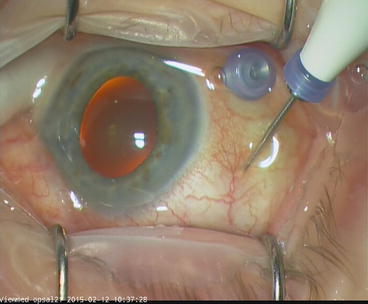
Fig. 3.1
Insertion of 27G trocars (DORC). Insert the infusion trocar as usual
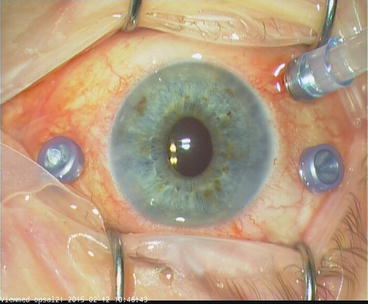
Fig. 3.2
Insert the instrument trocars towards 12 o’clock
Fig. 3.3
27G instruments are softer than 25G instruments. An insertion of trocars towards 12 o’clock facilitates the trimming of the vitreous base at the superior pole
27G instruments are softer than their 25G counterparts. A vitreous base shaving is rather difficult because the vitreous cutter is soft and bends when working in the periphery. A peripheral vitrectomy can be nonetheless performed without problems with exception of the superior pole from 11 o’clock to 1 o’clock. To overcome this problem, insert the superotemporal trocar towards 12 o’clock (instead towards 6 o’clock). Now the vitreous cutter bends less and you can reach easily the 12 o’clock position.
This problem only exists if you do not indent, e.g. if you do not work with chandelier light. If you insert a chandelier light, you can indent the vitreous base and remove it easily.
3.2 Valve Removal and Replacement (Figs. 3.4, 3.5 and 3.6)

Fig. 3.4
The valve has been removed
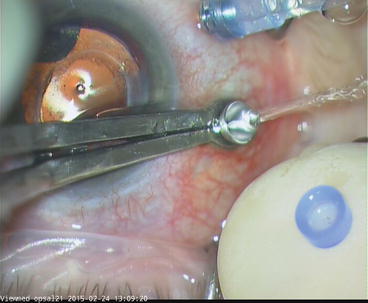
Fig. 3.5
Fixate the trocar with the trocar forceps. Place the valve on the tip of the index finger

Fig. 3.6
Then place the valve on the trocar
Fixate the trocar with the trocar forceps (DORC). Then remove the valve with an anatomic forceps. If you reattach the valve: Fixate the trocar with the trocar forceps, place the valve on your index finger and place the valve onto the trocar.
3.3 Removal of Trocar Cannulas (Figs. 3.7 and 3.8)
Fig. 3.7
Trocar removal. Remove the 27G trocar with a trocar forceps (DORC)

Fig. 3.8
Press against the sclerotomy with an anatomic forceps
It is useful to remove the trocars in the following order: first the instrument trocars, then the chandelier light and finally the infusion cannula. The infusion cannula remains in place until the end to avoid hypotension when removing the trocars. The infusion should therefore remain open until removal of the infusion cannulas.
To remove the trocars, pull out the trocar with the trocar forceps, and then press the edges of the sclerotomy together with a forceps and massage the sclerotomy with a cotton swab. Lastly the infusion cannula is removed. Before you do this, check the intraocular pressure manually.
If the globe is hypotensive after trocar removal, refill the eye with gas, until the eye is normotensive. Refill the eye before removing the infusion line and infusion trocar. In case of silicone oil, the eye should be rather hypotensive (approx. 8–10 mmHg). Then the infusion cannula with running infusion (BSS, air or oil) is removed. The sclerotomies are usually not sutured. Exceptions are silicone oil tamponades, because the oil may cause subconjunctival cysts.
A major advantage of not suturing a gas-filled eye is that the eyes are rarely hypertensive, as the expanding gas can escape postoperatively through the non-sutured sclerotomies. There is of course less leakage present with 27G compared with 23G. If you observe uveal tissue or even a vitreous prolapse out of the sclerotomy you should remove it with the vitreous cutter because otherwise there is a possible wicking and endophthalmitis risk. 27G sclerotomies require no suture.
3.4 Endoillumination
Endoillumination is essential for optimal visualization. Test different light sources, light probes and chandelier lights to achieve an optimal view to fundus.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


