Purpose
To describe ocular complications resulting from inverted insertion of a Kelman Multiflex anterior chamber intraocular lens (ACIOL).
Design
Retrospective observational case series.
Methods
We describe the outcomes of 4 cases of complicated cataract surgery in which a flexible open-loop polymethylmethacrylate (PMMA) ACIOL (Kelman Multiflex type) was placed in an inverted configuration, all of which were referred to a single institution.
Results
In all 4 cases, the placement of an inverted ACIOL resulted in ocular complications including chronic iritis, cystoid macular edema, pupil capture, iris adhesions, and corneal decompensation.
Conclusions
Inadvertent inverted placement of the Kelman Multiflex anterior chamber intraocular lenses can lead to a constellation of severe ocular complications. When inserting such lenses, the surgeon should ensure that the lens is correctly oriented such that the optic vaults anteriorly and not posteriorly.
The use of a flexible open-loop anterior chamber intraocular lens (ACIOL) (eg, Kelman Multiflex style) in the absence of capsular support during cataract surgery is well established, and the overall incidence of postoperative complications associated with their implantation is favorable when compared to techniques of implanting posterior chamber intraocular lenses via fixation of haptics to the iris or sclera. The Multiflex lens is designed to provide semi-compressible, 4-point haptic fixation, in order to reduce lens rotation in the anterior chamber, as well as forward vaulting of the optic, in order to maintain an adequate degree of clearance between the optic and the corneal endothelium anteriorly as well as the iris posteriorly. If inadvertently placed in an inverted configuration, such a lens would be predicted to have an abnormally anterior and unstable haptic placement and an undesirable posterior vault of the optic against the iris. We present the clinical outcomes of 4 cases of complicated cataract surgery in which a flexible open-loop polymethylmethacrylate (PMMA) Kelman Multiflex-style ACIOL was placed in an inverted configuration, resulting in a variety of early and late intraocular complications. All cases were referred to one of the authors (D.G.H.) of the Cornea Service, Department of Ophthalmology at the University of California, San Francisco (UCSF).
Report of Cases
Case 1
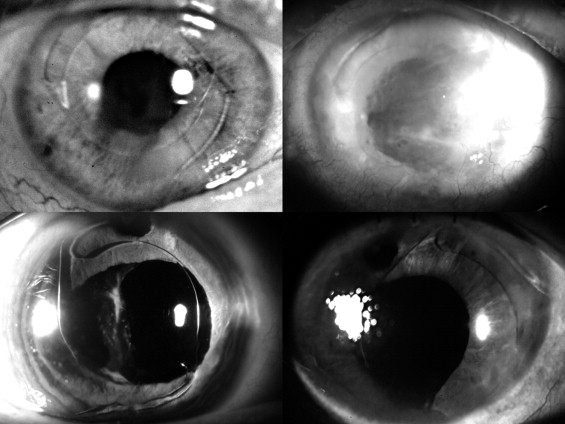
A 70-year-old man had cataract surgery with posterior capsular rupture followed by anterior vitrectomy and ACIOL placement in his right eye. Three weeks after surgery, the patient developed a retinal detachment in the operated eye, and a scleral buckle was placed. The patient presented to us 9 years later complaining of decreasing vision. His best-corrected visual acuity (BCVA) was 20/25, intraocular pressure was normal, and corneal pachymetry measured 730 μm. Slit-lamp examination revealed corneal edema and an inverted Kelman Multiflex-style ACIOL, which was bowed posteriorly into the iris ( Figure 1 , Top left). Ultrasound biomicroscopy revealed that the inferior haptic was in contact with the peripheral corneal endothelium. Specular microscopy showed significant loss of endothelial cells with an average cell density of 397 cells per mm 2 .
Because of the patient’s good visual acuity he was initially observed, but 9 months after initial presentation, the BCVA decreased to count fingers at 1 foot. Slit-lamp examination revealed diffuse corneal edema with epithelial bullae. Penetrating keratoplasty was performed along with ACIOL explantation followed by iris-sutured PCIOL implantation. Two years after penetrating keratoplasty, the BCVA remained stable at 20/30.
Case 2
A 76-year-old woman with a history of glaucoma and Ahmed valve placement in the left eye underwent complicated cataract surgery with posterior capsular tear, anterior vitrectomy, and ACIOL placement. The patient’s postoperative course was complicated by cystoid macular edema (CME) and iris capture of the optic with formation of synechiae. One year later, repositioning of the ACIOL and synechiolysis was performed along with a sub-Tenon’s injection of 40 mg of triamcinolone acetonide. Postoperatively, the patient’s BCVA was 20/80 with persistent CME and peripheral corneal edema corresponding to the area overlying the Ahmed valve tube tip. The patient’s corneal edema progressively worsened with drop in vision to count fingers at 3 feet.
The patient was referred to us 5 years after her initial cataract surgery for worsening pain in the left eye. On ocular examination, her BCVA was count fingers at 6 inches. Central corneal thickness was 950 μm, and slit-lamp examination revealed diffuse corneal edema with large epithelial bullae. The tip of the Ahmed valve in the anterior chamber appeared to be in close proximity to the corneal endothelium. The Kelman Multiflex ACIOL was in an inverted configuration with the haptics and optic compressed posteriorly against the iris ( Figure 1 , Top right).
The patient first underwent repositioning of the Ahmed tube given the presumption that the tube location may have been contributing at least in part to the corneal decompensation. Although a subsequent penetrating keratoplasty with intraocular lens exchange was planned for the patient, she was unable to obtain medical clearance for this procedure because of a decline in her health. Because of pain secondary to pseudophakic corneal edema and questionable visual potential in the affected eye, the patient elected to undergo a Salleras procedure (corneal cautery), which resulted in good relief of her pain.
Case 3
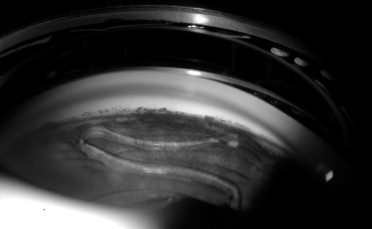
A 78-year-old woman underwent cataract extraction with posterior capsular rupture, zonular dehiscence, anterior vitrectomy, and ACIOL placement in her right eye in 2005. She was seen by us 4 months after surgery for a second opinion. Her BCVA was 20/50 with a normal intraocular pressure. Slit-lamp examination showed a clear cornea with an upside-down Kelman Multiflex ACIOL vaulting posteriorly against the iris ( Figure 1 , Bottom left, and Figure 2 ). Optical coherence tomography (OCT) revealed evidence of CME.
The patient underwent ACIOL explantation and implantation of a PCIOL using a McCannel fixation technique, accompanied by intravitreal injection of triamcinolone acetonide. At the 1-month follow-up visit, the patient’s BCVA was 20/50 and the sutured PCIOL appeared to be in good position. There was some persistence of CME, and treatment for this was initiated. The patient was then lost to follow-up.
Case 4
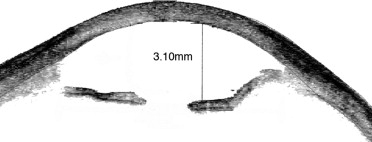
A 66-year-old woman had undergone cataract extraction with posterior capsular tear, anterior vitrectomy, and ACIOL placement in her left eye the week prior to her presentation in 2007. Her BCVA was counting fingers at 2 feet, and central corneal thickness measured 903 μm. On follow-up 2 months later slit-lamp examination revealed an inverted Kelman Multiflex ACIOL with the haptics resting on the cornea and the iris in a posteriorly convex position ( Figure 1 , Bottom right) as evidenced on anterior-segment OCT ( Figure 3 ). Three months after her initial presentation, the patient underwent IOL exchange with a scleral-sutured PCIOL. Descemet stripping automated endothelial keratoplasty was performed 2 months later because of nonclearing corneal edema. Three months following endothelial keratoplasty, her vision had improved to 20/30, a level that was maintained 2 years later.