Chapter 30
UNIQUE ASPECTS OF TRAUMA IN CHILDREN

Caring for children with ocular trauma involves several unique aspects such as:
• the possibility of prenatal injuries (e.g., ocular penetration by an amniocentesis needle1);
• predisposition to certain types of trauma (e.g., fireworks or toys related);
• diagnostic challenges due to limitations experienced during history taking and examination (see Chapter 9);
• the developing visual system and the potential for amblyopia;
• an orbit that is immature (cosmesis following enucleation or evisceration; see Chapter 31);
• the potential of eyes healing differently than adults’ eyes, affecting surgical decision making; and
• the sensitivity in families and society toward suffering children, extending far beyond physical pain and disability.2
EPIDEMIOLOGY AND PREVENTION
The reported proportion of ocular injuries occurring in children varies according to study design,a population, and cultural and economic influences on admission rates. Based on data in the United States:
• children are involved in 16 to 34%3–6 of trauma-related hospitalizations;
• the estimated inpatient hospitalization incidence rate is 15/100,000/year7;
• 21% of visits for ophthalmic trauma emergency care are by those under 158;
• 24% of all serious ocular injuries occur in those under 15 (USEIR).
The rates are similar, even higher, in some studies from other countries:
• 38% in a 12-year review of eye trauma admissions in Belfast9;
• 47% in Israel10;
• 47% in South India11;
• 35% in Helsinki12;
• 25% in Melbourne.13
Virtually all studies of pediatric ocular trauma show a male preponderance, which increases with age. Male/female ratios in the USEIR in 1998:
• 0–5 years: 1.9:1;
• 6–10 years: 3.4:1;
• 11–15 years: 5.1:1.
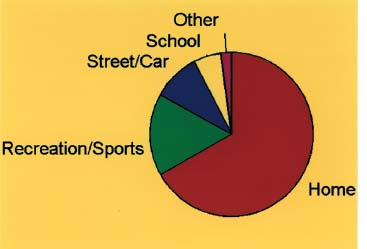
Forty-two percent of open globe injuries in patients younger than 15 years were found to have a poor prognosis.14 The places and sources vary (Figs. 30–1 and 30–2).
• Sports and recreation, sticks, and toys. These represent a major etiology worldwide,4,7,10,15–18 and the injuries are almost always preventable with adult supervision. Use of proper eye/facial protectors can reduce the rate of sports injuries. In the United States, baseball is a major cause of serious ocular19–21 and dental/facial trauma.22,23 Mandating softer baseballs and faceguards for batters is very effective24–26; facial protectors in youth league hockey in Canada and the United States resulted in a 50% annual reduction in blind eyes.27,28 Noncompliance with regulations remains responsible for continued ocular injuries.29 Parents and children must be educated about eye protection for sports; the protectors have been standardized (ASTM)29 and, after tests by independent laboratories,30 certified for the consumer.
• Nonpowder firearms, such as paintball guns, BB guns, pellet air guns, toys that fire projectiles, and some exotic projectile-firing devices (Figs. 30–3A–D, and 30–4A, and B). Of 32,000 such injuries in the United States each year, about 8% involve the eye with 60% of these patients being children.32,33 Representing 5% (USEIR) to 7%34,35 of all serious ocular injuries where air gun use is relatively unrestricted, the consequences are often dire.34 A war game involving shooting gelatin-coated paint capsules with up to 90 m/s speed at the opponent, paintballing is increasingly popular in North America36 and Europe. Eye injuries almost always occur when the victim is not wearing facial protection in an unsupervised environment.37,38
• Fireworks. In the EIRA, fireworks are responsible for 4.4% of all injuries and 80% of these are caused by bottle rockets.39 Legislative action appears to be an effective means of controlling injuries from fireworks.39,40 States that prohibit consumer fireworks sales have a much lower incidence of ocular injury from this source compared with states with less regulation.41 U.S. and South African data have demonstrated an increased number of fireworks-related ocular injuries occurring after a legislative repeal of a ban on consumer fireworks sales.22,43
PEARL… It is crucial to educate parents of monocular children, regardless of age, gender, or refractive error, about the use of safety eyewear during sports.31
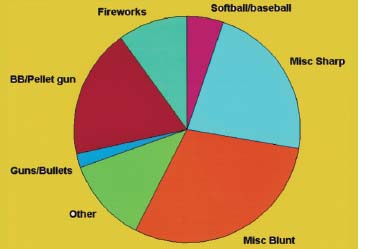
FIGURE 30–2 Source of injury for patients <15 years of age (USEIR). In 2212 reports listing the source of injury for this age group, large proportions of injuries were due to BB/pellet guns (18%), fireworks (10%), and softball/baseball (5%).
EVALUATION
The history of even serious pediatric ocular injury can be dubious because:
• the child’s account is often vague owing to poor insight into the situation or deceptive in an effort to avoid punishment; and that
• usually there is no (available) adult eyewitness. The ophthalmologist should maintain a high index of suspicion for trauma that is less obvious (e.g., occult open globe injury or penetrating orbital injury; see Figs. 30–3 and 30–4 and Chapters 9, 10, and 15). Recognizing the presence and extent of tissue damage must be weighed against exacerbating the situation if the child is combative or there is severe lid hemorrhage (see Chapter 8). A careful consideration of the risks is necessary in deciding whether to immobilize the child forcibly (assistants, blankets, papoose board; see Fig. 30–5) and pry open the lids versus using diagnostic sedation/general anesthesia (Table 30–1).


FIGURE 30–3B A 14-year-old male with severe orbital injury from accidental discharge of the device.
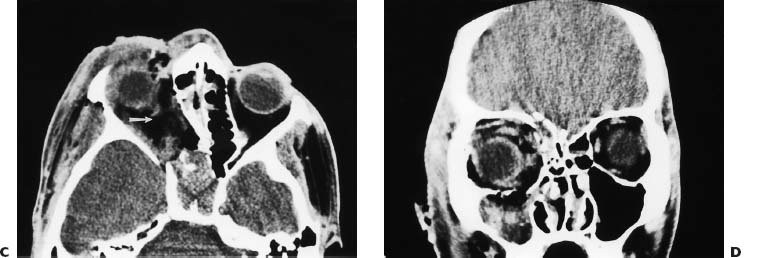
FIGURE 30–3 (C and D) CT scans demonstrate fracture of all walls of the orbit, optic nerve avulsion (arrow), and diffuse infiltration of the orbit with organic debris (potato).
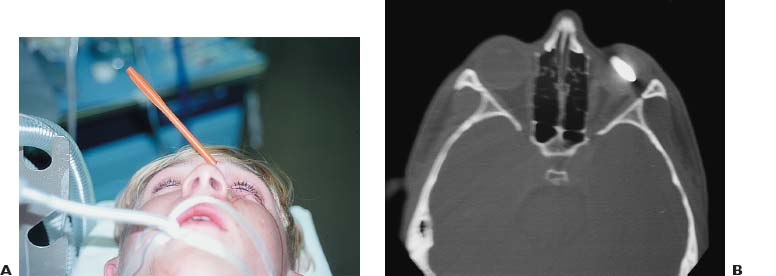
FIGURE 30–4 (A and B) Perforating wound due to a toy arrow fired from a crossbow. (Photograph courtesy of Rick Burgett, MD.)

PEARL… Children are especially prone to the oculocardiac reflex (Fig. 30–6), and any young patient presenting with bradycardia, nausea, somnolence, and/or syncope should be suspected of having such a reaction.
The differential diagnosis in case of a vomiting child with facial trauma includes:
• intracranial injury;
• increased IOP (e.g., from hyphema; see Chapters 17 and 20);
• uveal injury (see Chapter 16);
• extraocular muscle entrapment (see Chapter 36); and
• retrobulbar hemorrhage (see Chapter 12).

FIGURE 30–6 A 9-year-old boy hit by a pitched baseball. Coronal CT image demonstrates a left orbital floor trap-door fracture with entrapment of tissue around the inferior rectus and fluid in the left maxillary sinus. Sustained nausea and vomiting followed the injury, which prompted repeated visits to the ER and neurosurgical admission. When vomiting had not subsided 24 hours after admission, oculocardiac reflex was suspected; the orbit was explored and the fracture repaired. Nausea and vomiting resolved immediately after surgery. (Photograph courtesy of Rick Burgett, MD.)
| Wake child |
| Have the child sit with a parent |
| Give the child a token gift, such as a colorful sticker, prior to examination |
| Approach in a nonthreatening manner; forced cooperation almost never works |
| Talk directly to the child in a calm, soft voice |
| Explain the anticipated procedures to the child before acting |
| Assure the child that you will not hurt him or her |
| Remove white lab coats because some children are intimidated by them |
| Crying children are more likely to open their eyes if the room is darkened; this may allow you to assess chamber depth and media clarity |
| Keep the ophthalmoscope’s light intensity to a minimum |
| Sedation |
| Oral dose of chloral hydrate44 80–100 mg/kg for the first 20 kg of body weight, supplemented as necessary with a one-time dose of 40 mg/kg; the child must be <6 years or >20 kg body weight and NPO for 4 hours; pulse oximetry and blood pressure should be monitored throughout |
| General anesthesia |
| Brief mask anesthesia for short procedures such as superficial foreign bodies |
| Intubation if longer procedure such as suturing open wounds is expected |
* See also Chapter 9.
INJURIES WITH SPECIAL IMPLICATIONS
Intraocular Hemorrhages in the Neonate and Infant and Shaken/Battered Baby Syndrome
Intraretinal hemorrhages occur in ≤30% of cases of cesarean births and may take up to 2 weeks to resorb. Periretinal hemorrhages are especially important among infants <2 years of age as they are the most susceptible to injury by shaking.
The ocular (and/or intracranial) findings in the shaken/battered baby syndrome (see Chapters 10 and 33) may occur in the absence of obvious external injury and include:
• intraretinal and subhyaloid/submembranous hemorrhages (hemorrhagic macular cystb), usually most dense at the posterior pole45 (see Figs. 30–7 to 30–9);
• subretinal hemorrhage;
• vitreous hemorrhage (called Terson’s syndrome if related to intracranial bleeding; may be associated with significant retinal and visual cortical pathology47);
• retinoschisis;
• retinal detachment;
• circular perimacular folds (Fig. 30–9)48–51; and
• optic nerve hemorrhage.
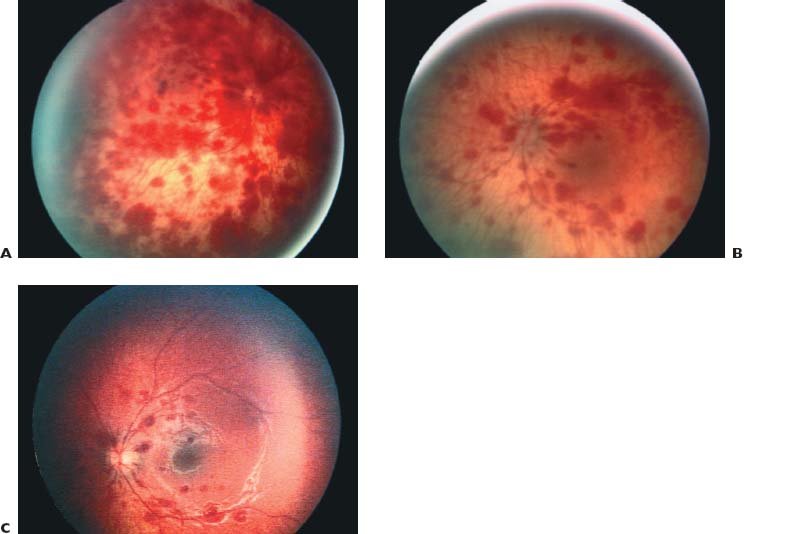
FIGURE 30–7 (A–C) The spectrum of intraretinal hemorrhages in shaken baby syndrome.
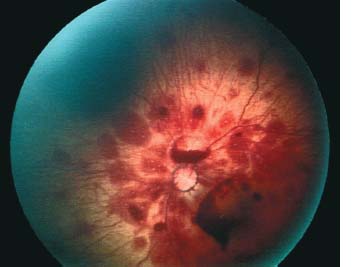
FIGURE 30–8 Large boat-shaped preretinal hemorrhages in shaken baby syndrome.
PEARL… Although typically bilateral, nonaccidental retinal hemorrhages may be asymmetric or even unilateral.46
Despite surgical removal of the vitreous hemorrhage, vision commonly remains severely impaired because of cerebral dysfunction52 or macular damage. Peripheral retinoschisis has been associated with high mortality.49
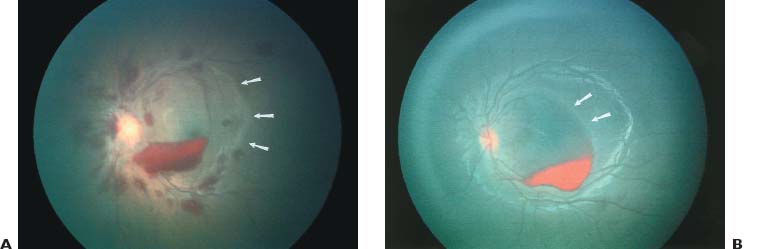
FIGURE 30–9 (A and B) Temporal macular fold (arrows) caused by submembranous hemorrhagic macular cyst in shaken baby syndrome.
The pathomechanism of intraocular hemorrhages in shaken baby syndrome is controversial. Major external trauma may result in relatively minor ocular consequences.c Compression of the chest may raise the intracranial venous pressures and produce Purtscher’s retinopathy (see Fig. 30–10 and Chapter 33).53 Shearing produced by multiple sequences of acceleration and deceleration when an infant is shaken54,55 disrupts both intracranial and intraocular vessels, and a vitreous gel that is adherent to the infantile retina may explain not only the hemorrhages but also the formation of retinal detachment or retinoschisis.51
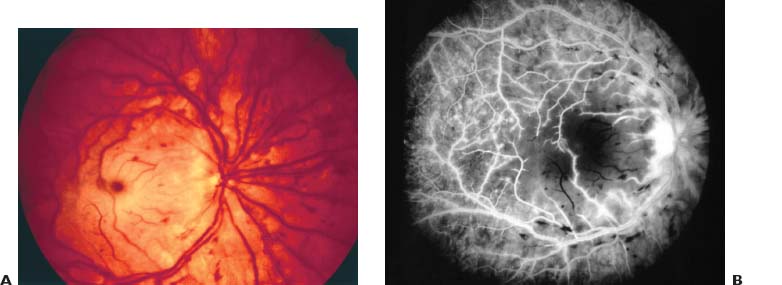
FIGURE 30–10 Purtscher-type retinopathy with no apparent head trauma in an 8-year-old male thrown from an all-terrain vehicle. (A) Color fundus photograph (B) FA.
PEARL… Since an estimated 40% of eyes show clinically visible pathology,45 the ophthalmologist plays a pivotal role in the identification of child abuse (see Table 30–2).
Falling from a bed is insufficient to produce retinal hemorrhages; being “clumsy” does not account for orbital and lid ecchymoses. It is the eye care professional’s moral and legal responsibility to report the incident for further investigation (see Chapter 7).
| Retinal, subhyaloid, and vitreous hemorrhages |



