3 Understanding Geriatric Syndromes, the Geriatric Interdisciplinary Team, and Resources to Optimize Care for Older Patients
 Introduction
Introduction
Otolaryngologists, like all specialist physicians in any aging society, face important challenges in effectively caring for older adults. Effective care requires looking beyond the bounds of otolaryngology to develop an understanding of frailty, multimorbidity, and geriatric syndromes that intersect with otolaryngological conditions. This clinical knowledge provides the foundation for geriatric competence, affording a better capacity to collaborate with the geriatric interdisciplinary team (GIDT) as well as to target and access resources for older patients. As a result, geriatric patients and their family caregivers benefit from better integrated and coordinated care as well as from GIDT surveillance to reduce unmet needs and avoid complications.
Aging societies bear an increasing burden of health care need that emerges from the intertwined forces of elder dependency and compression of morbidity.1–4 Elder dependency occurs as more people live longer while birth rates decline. This extension of life with reduction in births creates a larger proportion of dependent older people to younger people who provide the economic base as well as care for elders.5 Dependent elders are those who, in demographic terms, no longer contribute economically to society. Underlying that dependency are implicit concerns of frailty and multimorbidity. However, compression of morbidity may mitigate dependency by moving time of greatest need closer to the point of death.1,3 Consequently, the demographic of an aging society creates manifold and dynamic consequences for health and social care needs.5 At the population level, frailty and multimorbidity contribute to both volume and complexity in care of older patients. Nonetheless, not all consequences in an aging society are easily and clearly projected.1,6 Thus specialist physicians, as with all clinicians who are not specialists in the care of older people, benefit from preparation that supports competent practice in the rapidly evolving context of an aging society.
Geriatric competence describes the application of requisite knowledge for safe, effective, and quality care for older adults. The Institute of Medicine, along with authors from geriatric medicine and nursing, explicitly outlines that continued inattention to the unique characteristics and resultant needs of older adults in education and practice generates dire present and future consequences to health care and to society.7–9 The Institute of Medicine amalgamated a vast collection of literature addressing the care of older adults, calling for a “retooling” of American clinical education, health care training, and care delivery.7 This report established the current foundation for enacting geriatric competence as a requirement, and not an option, for all clinicians caring for older adults.
Geriatric competence broadly includes knowledge of aging as an integral biological, psychological, and social process; the functional consequences of aging along with diseases, conditions, and syndromes common to later life; and the means to recognize and mitigate the risks of adverse events in the care of older people. Specific competencies, which are particular to individual disciplines, are reliant on social contract and scope of practice. The Association of American Medical Colleges (AAMC) enacted a set of geriatric competencies for medical students, contemporaneously with the Institute of Medicine’s Retooling for an Aging America report.7,8 The AAMC requires that graduating medical students possess the following competencies: medication management; cognitive and behavioral disorders; self-care capacity; falls, balance, and gait disorders; health care planning and promotion; atypical presentation of disease; palliative care; and hospital care for elders.8 Each of these competencies is detailed in the Appendix of this chapter.
Practice in an aging society requires otolaryngologists then to look beyond their own specialty care toward geriatric competence. As clinicians who do not specialize in aging, otolaryngologists must achieve competence through both knowledge and collaboration. The larger aim is to coordinate care and integrate resources to optimize care quality, safety, and patient and family satisfaction. This chapter describes the elements necessary to achieve that optimal level of care for older patients.
Three elements are necessary in order for otolaryngologists to optimize care for older adults. First, knowledge of important clinical phenomena that are common to older adults enables the otolaryngologist to identify the interface between these clinical conditions and otolaryngological diseases, conditions, and syndromes as well as to target areas for collaboration with the GIDT. Second, familiarity with roles and responsibilities with the geriatric interdisciplinary team as well as colleagues who can offer collaboration when a GIDT is not available enables the otolaryngologist to promote care coordination, ensure transitional care, and avoid fragmentation. Both knowledge of geriatric phenomena and collaboration with a GIDT or geriatric colleagues require routine continuing education and the savvy use of geriatric resources. Third, knowledge of and means to access local and national resources for continuing clinician education, for patient education and services, and for family support streamlines otolaryngological care for older adults as well as support for their family caregivers. The chapter concludes with a summary of implications for future geriatric otolaryngology practice, education, and research in the context of our aging world.
 Frailty, Multimorbidity, and Geriatric Syndromes
Frailty, Multimorbidity, and Geriatric Syndromes
Conditions and syndromes of very late life are characterized by intricate biological, physical, and psychological processes that intersect and commonly cascade, resulting in functional decline at all levels. As a result, clinicians face assessment and identification of subtle, complicated phenomena despite relatively straightforward presenting complaints among older adults. Frailty is increasingly understood as playing a critical role in this intersecting cascade that results in several etiologies converging in intersecting pathogenesis and leading to syndromes common to frail older adults.10–12 These conditions emerge from cascading etiologies and are generally termed geriatric syndromes. There is no common definition for geriatric syndromes.10 Geriatric syndromes, whereas they have multiple intersecting etiologies, have a complex manifestation with observable hallmarks like falls or pressure ulcers. Whether “frailty” is a geriatric syndrome as are “falls” and “incontinence” or whether it stands alone as a syndrome that contributes to others is not yet clear from extant evidence.10,11 Nonetheless, the issues of complex and intersecting pathogenesis and presentation along with risks of disability and continuing care needs are well established.10–13 Inouye and colleagues, in a classic work, demonstrate the complexity that characterizes geriatric syndromes in a widely known figure (Fig. 3.1).10
Frailty is ever better understood as an expression of aging processes that result in declining functional reserve. Clegg and colleagues vividly depict the distinction between fit and frail elders (Fig. 3.2). Declining reserves lead to vulnerability, which magnifies the effects of insults, resulting in deleterious events like a fall, disability, and escalating needs for care.12 Although debate continues over whether frailty emerges from phenotypic flaws13,14 or multiple deficits accumulated over time,15,16 vast evidence points to the manifest impact on older individuals and on aging societies. Clegg and colleagues schematize the pathophysiology of frailty, clearly outlining the relationships from the cellular to the social levels in this epigenetic phenomenon from which geriatric syndromes and functional debility in late life emerge (Fig. 3.3).11
Classification of geriatric syndromes remains somewhat confusing. There is no universal and widely accepted definition or definitive list that might guide nonspecialist clinicians. Geriatric syndromes may be more easily understood if classified into antecedent and consequent syndromes. Specifically, some geriatric syndromes like frailty and sarcopenia seem to presage declining constitutional reserve.11 In essence, these syndromes are characterized by declining reserve at the level of cells and tissues (e.g., muscle function in sarcopenia) that then contribute to clinically manifest syndromes like osteoporosis and potentiate normal aging changes like presbystasis. The result is consequent syndromes like falls. In this example, falls are obviously connected to sarcopenia, presbystasis, and osteoporosis. However, falls result from functional effects of sarcopenia, presbystasis, and sometimes osteoporosis, whereas osteoporosis also exacerbates risk of injury from falls. All of the syndromes implicated here converge in the clinical manifestation of the apparently simple syndrome of falls in older adults. Moreover, a fall event also results in risk for other syndromes like delirium and pressure ulcers and engenders the need for an array of health and social care services in the frail older adult.12 In general, consensus regarding geriatric syndromes suggests that, at minimum, falls, fear of falling, incontinence, pressure ulcers, sleep disorders, and anorexia with failure to thrive are included in the classification.
Importantly, frail older adults experiencing geriatric syndromes are likely to be multimorbid, a term describing the state of sustained, multiple comorbid conditions. Older adults are widely acknowledged, both in epidemiological studies and in clinical wisdom, as often presenting with a constellation of chronic, noncommunicable diseases and conditions that coexist. These coexistent diseases and conditions complicate presentation, assessment, treatment, and outcomes.17,18 Nonetheless, the presence of comorbid conditions as the phenomenon now termed multimorbidity is incompletely studied.17 Physiological connections between frailty and multimorbidity are poorly elucidated as are the contributions of social determinants of health. Social determinants of health obviously influence development of chronic noncommunicable disease, which accounts for the major burden of health care globally.17,19 Social determinants of health may also aggravate the antecedents and consequences of frailty and geriatric syndromes.12 However, definitive investigation of the interrelationships of frailty, multimorbidity, and geriatric syndromes is as yet unreported in the world literature on aging. As a result, erudite clinicians must remain aware of the risks and consequences of this aging triad, pursuing developing evidence with the goal of optimizing clinical care.
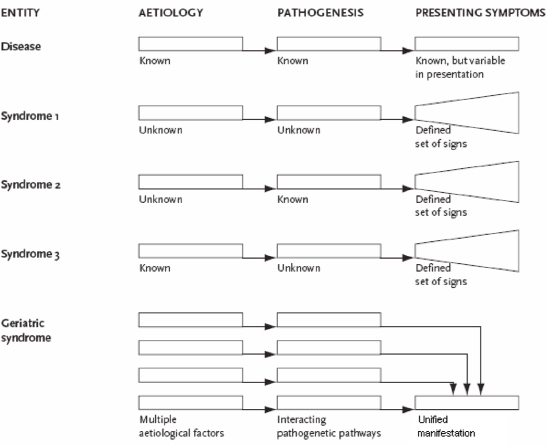
Fig. 3.1 Schematic conceptual representation of clinical conditions defined by the terms disease, syndrome, and geriatric syndrome, illustrating differences in numbers and complexity of relevant factors, including etiological risk factors, pathophysiological mechanisms, and presenting symptoms. (Used with permission from Inouye SK, Studenski S, Tinetti ME, Kuchel GA. Geriatric syndromes: clinical, research, and policy implications of a core geriatric concept. J Am Geriatr Soc 2007;55(5):780–791.)
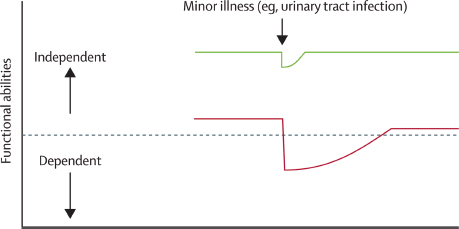
Fig. 3.2 Vulnerability of frail elderly people to a sudden change in health status after a minor illness. The green line represents a fit elderly individual who, after a minor stressor event such as an infection, has a small deterioration in function and then returns to homoeostasis. The red line represents a frail elderly individual who, after a similar stressor event, undergoes a larger deterioration, which may manifest as functional dependency, and who does not return to baseline homeostasis. The horizontal dashed line represents the cutoff between a dependent and an independent functional status. (Used with permission from Clegg A. The frailty syndrome. Clin Med 2011;11(1):72–75.)

Fig. 3.3 Schematic representation of the pathophysiology of frailty. (Used with permission from Clegg A. The frailty syndrome. Clin Med 2011;11(1):72–75.)
The exemplar geriatric syndrome used here, falls, illustrates critical aspects of the intersections of frailty, multimorbidity, and geriatric syndromes for otolaryngological practice. In this case, the otolaryngologist possesses the expertise necessary to address presbystasis20 as a major factor resulting in fall risk and actual falls for any given older patient. This exemplar further underscores the interdisciplinary and collaborative nature of optimal geriatric care. In this case, best practice warrants fall risk assessment, fall event grading, and investigation of fear of falling syndrome, depending on the individual presentation.21,22
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


