Purpose
To evaluate the usefulness of ultrasound biomicroscopy in confirming intraocular lens haptic–induced ocular irritation and in the management of these patients.
Design
A retrospective review of patient data.
Methods
Twenty pseudophakic patients who underwent ultrasound biomicroscopy examination between May 2009 and February 2011 to confirm the clinical suspicion of misplacement of intraocular lens haptics were reviewed. Ophthalmic findings at the time of presentation and at each follow-up visit, and management of each patient, were recorded.
Results
Intraocular lens haptic misplacement was confirmed by ultrasound biomicroscopy in all suspected cases. In 75% of the eyes 1 haptic was embedded in the iris; it extended into the ciliary body process in 35% and into the pars plana in 10%. Focal iris thinning/atrophy was detected by ultrasound biomicroscopy in 15% of cases and focal angle closure in 25%. Intraocular lens exchange was performed in 40% of patients. The remaining 60% were kept under observation, with the addition of topical steroids and/or cycloplegics in eyes that demonstrated anterior chamber inflammation and intraocular pressure–lowering medications in eyes with persistent elevated intraocular pressure or glaucoma.
Conclusions
Ultrasound biomicroscopy appears to be a valuable tool in confirming the presence of haptic-induced ocular irritation and in assisting the management of these patients.
Cataract surgery has greatly evolved in the past few decades. The development of new intraocular lens (IOL) designs and materials, along with advancements in phacoemulsification technique, have led to successful outcomes in the majority of patients.
Complications related to IOL position are occasionally seen, but not as frequently as in the past, owing to the predominance of posterior chamber IOL implantation in the capsular bag. In the setting of posterior capsule rupture, sulcus implantation remains a common option in patients with adequate capsular support. A concern with this approach is the close proximity of the IOL to the iris. It is often difficult to precisely determine the correct placement of the haptics in the sulcus. Chafing or erosion of the iris may occur, particularly with misplaced haptics, which may lead to complications such as IOL-induced chronic postoperative inflammation. Anterior chamber IOLs have long been associated with intraocular inflammation, pseudophakic bullous keratopathy, glaucoma, and lower visual acuity outcomes. However, more recent studies have revealed a decrease in incidence of complications associated with redesigned, open-loop anterior chamber IOLs.
Ultrasound biomicroscopy (UBM) is a noninvasive tool that allows visualization of the anatomic relationships of anterior segment structures, including position of the IOL and haptics, producing images with a resolution of approximately 40 μm.
We present the ophthalmic and UBM findings of 20 patients suspected of having chronic inflammation secondary to misplaced IOL haptics on clinical assessment, and discuss the management of such cases.
Methods
To confirm the clinical impression of misplaced IOL haptics, we retrospectively reviewed the medical records of 20 pseudophakic patients who underwent UBM examination using a 50-MHz probe between May 9, 2009 and February 8, 2011 at Cleveland Clinic Cole Eye Institute. The study was approved by the Cleveland Clinic’s Institutional Review Board and followed the tenets of Declaration of Helsinki.
All patients were referred to our institution for investigation and management of postphacoemulsification chronic unilateral inflammation, unilateral recurrent hyphema, increased intraocular pressure (IOP), recurrent vitreous hemorrhage, or a combination of those. None of the patients were suspected of having misplaced haptics as the cause of their inflammation. The position of the IOL haptics and their relationships to the surrounding anterior segment structures were determined by UBM. Ophthalmic findings at the time of presentation and at each follow-up visit were recorded, and management of each patient was further reviewed.
Results
Mean patient age at presentation to our institution was 68.1 ± 11.2 years. There were 16 male and 4 female patients. Time from cataract surgery to referral/diagnosis of misplaced haptics by UBM ranged from 1-288 months (mean 59 ± 69 months). Initial surgical procedure was phacoemulsification for all patients. Intended IOL placement was in the sulcus in 10 eyes (50%) and in the bag in 8 eyes (40%). One eye (5%) had iris-sutured posterior chamber IOL and 1 (5%) had an anterior chamber IOL ( Table 1 ). Posterior capsule was reported to be intact only in the eyes that had IOL implanted in the bag. Type of IOL implanted varied according to anatomic location of planned implantation. Patients with in-the-bag implants received single-piece acrylic IOLs, whereas patients with sulcus implantation received multi-piece acrylic IOLs.
| Eye | IOL Location | UBM Findings | Time (Months) |
|---|---|---|---|
| 1 | In the bag | One haptic not in bag, rubbing against iris (thinning of the iris) | 108 |
| 2 | In the bag | One haptic not in bag, rubbing against central and peripheral iris (thinning of the iris) | 24 |
| 3 | In the bag | One IOL haptic pushing iris toward angle, focal angle closure | 84 |
| 4 | In the bag | Both haptics eroding into peripheral iris (thinning of the iris) | 66 |
| 5 | Sulcus | One haptic embedded in the iris | 144 |
| 6 | Sulcus | Both haptics embedded in the iris | 2 |
| 7 | Sulcus | One haptic eroding iris, second haptic extending into ciliary body | 120 |
| 8 | In the bag | One haptic out of capsular bag, extending into pars plana | 27 |
| 9 | Sulcus | One haptic embedded in the iris | 7 |
| 10 | Sulcus | One haptic embedded in the iris, focal angle closure | 8 |
| 11 | Sulcus | One haptic embedded in the iris, focal angle closure | 3 |
| 12 | In the bag | One haptic out of bag, embedded in the iris, pushing iris anteriorly | 36 |
| 13 | Sulcus | One haptic embedded in the iris, focal angle closure | 83 |
| 14 | In the bag | One haptic out of bag, extending to ciliary body | 98 |
| 15 | Sulcus | One haptic extending into ciliary body | 1 |
| 16 | Sulcus | One haptic extending into ciliary body | 20 |
| 17 | Iris sutured | One haptic extending into pars plana | 18 |
| 18 | Sulcus | One haptic pushing iris anteriorly, 1 haptic extending into ciliary body | 288 |
| 19 | In the bag | One haptic extending into ciliary body, 1 haptic pushing iris anteriorly, focal angle closure | 3 |
| 20 | ACIOL | One haptic transecting iris peripherally, extending into ciliary body | 40 |
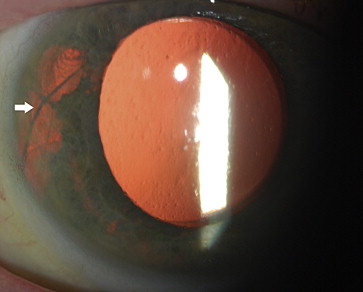
Presenting ocular features of the 20 involved eyes are summarized in Table 2 . Twelve patients (60%) had a history of chronic unilateral postoperative inflammation, with extensive negative examination for uveitis etiology. Eight patients (40%) had recurrent episodes of hyphema. History of elevated IOP or glaucoma was found in 13 eyes (65%). History of recurrent vitreous hemorrhages was elicited in 10 patients (50%). Cystoid macular edema was present in 4 eyes (20%), demonstrated by optical coherence tomography. Iris transillumination defects ( Figure 1 ) were observed in 6 eyes (30%).
| Eye | Chronic Inflammation | Hyphema | VH | Elevated IOP | CME | TID | Management |
|---|---|---|---|---|---|---|---|
| 1 | No | Yes | Yes | Yes | No | Yes | PPV, IOL exchange, ACIOL |
| 2 | Yes | Yes | Yes | No | No | Yes | PPV, IOL exchange, ACIOL |
| 3 | No | No | No | Yes | No | Yes | Observation, IOP managed medically |
| 4 | Yes | No | Yes | No | No | No | Observation |
| 5 | Yes | No | No | Yes | No | No | IOP managed medically |
| 6 | No | Yes | Yes | Yes | No | Yes | IOP managed medically |
| 7 | No | No | Yes | No | No | Yes | PPV, IOL exchange, sutured IOL |
| 8 | No | Yes | Yes | Yes | Yes | No | PPV, IOL exchange, sutured IOL, IOP managed medically |
| 9 | Yes | No | No | Yes | Yes | No | Observation, topical steroids, IOP managed medically |
| 10 | Yes | No | No | Yes | No | Yes | PPV, IOL exchange, sutured IOL, IOP managed medically |
| 11 | Yes | No | No | No | No | No | Observation, topical steroids, cycloplegics |
| 12 | Yes | Yes | Yes | No | No | No | Observation |
| 13 | Yes | No | No | Yes | No | No | Observation, prior history of glaucoma tube shunt surgery |
| 14 | No | No | Yes | Yes | No | No | Observation, IOP managed medically |
| 15 | Yes | Yes | No | Yes | No | No | Observation |
| 16 | Yes | No | No | Yes | No | No | Observation, topical steroids, IOP managed medically |
| 17 | No | Yes | Yes | Yes | Yes | No | PPV, IOL exchange, sutured IOL |
| 18 | Yes | Yes | Yes | Yes | No | No | PPV, IOL exchange, sutured IOL |
| 19 | Yes | No | No | No | No | No | Observation |
| 20 | No | No | No | No | Yes | No | PPV, IOL exchange, sutured IOL |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


