Chapter 9 Tympanoplasty—Outer Surface Grafting Technique
 Videos corresponding to this chapter are available online at www.expertconsult.com.
Videos corresponding to this chapter are available online at www.expertconsult.com.
HISTORICAL ASPECTS
Systematic reconstruction of the tympanic membrane, the sine qua non of the modern era of reconstructive ear surgery, had its beginning with reports by Wullstein1 and Zollner.2 Split-thickness or full-thickness skin was placed over the de-epithelialized tympanic membrane remnant. The initial results were very encouraging, but graft eczema, inflammation, and perforation were common.
As a result of these experiences, most surgeons had begun changing to undersurface (underlay) connective tissue grafts by the late 1950s (see Chapters 11 and 12). The House Clinic physicians continued using an onlay technique, but changed to “canal skin,”3,4 which actually was periosteum graft covered by canal skin. This change was made in 1958, and resulted in an immediate improvement in results. Draining ears and total perforations continued to have a failure rate reaching 40%.
In 1961, Storrs5 published the results of a small series of cases in which temporalis fascia had been used as an outer surface graft. Changing to this technique resulted in a dramatic improvement in results over the next 3 years: greater than 90% graft take.6–8
PATIENT SELECTION AND EVALUATION
Let us assume, for purposes of this chapter, that the patient has a dry central perforation. The ear may drain briefly with upper respiratory infections or if water is allowed to get into the ear. This discharge responds promptly to local medication. The preoperative treatment of the draining ear is discussed in depth in Chapter 16. When one is dealing with a dry central perforation, or inactive disease, surgery is elective, and the patient (or family) should be so informed. Assuming that the problem is unilateral, with only a mild hearing impairment, the only indication for surgery is to avoid further episodes of otorrhea.
When contemplating tympanoplasty, the House Clinic physicians do not usually test to determine the status of the eustachian tube.9 The philosophy has been that tubal malfunction per se is not a contraindication to tympanoplasty, but that the operation would not be successful unless tubal function is re-established. Many patients showing no tubal function by various available tests used in the past have been operated on to eliminate a chronic drainage problem. When the ear heals, the drum is usually mobile. Re-exploration in some of these patients has shown normal mucosa in the tubotympanum, where before surgery the mucosa was of a very poor quality. It would seem that the surgery, in eliminating infection and sealing the ear, is in itself the best treatment for the obstructed tube.
PATIENT COUNSELING
What is the outlook with surgery, and what are the risks and complications? A surgeon must relate his or her own experience. House Clinic physicians explain that the likelihood of obtaining a permanently healed, dry ear, which may be treated normally, is better than 90%. “The only complication that happens with any degree of regularity, and is serious, is a total loss of hearing in the operated ear. That likelihood is no more than 1%. All of the other things listed here are either very remote or are temporary.” (“Listed here” refers to the Risk and Complications section of a patient Discussion Booklet. The Risk and Complications Sheet is given to the patient at the time the surgery is scheduled, which allows the patient to review the sheet leisurely. Appendix 1 is the Risk and Complications Sheet.)
PREPARATION IN THE OPERATING ROOM
Arrangement and Instrumentation
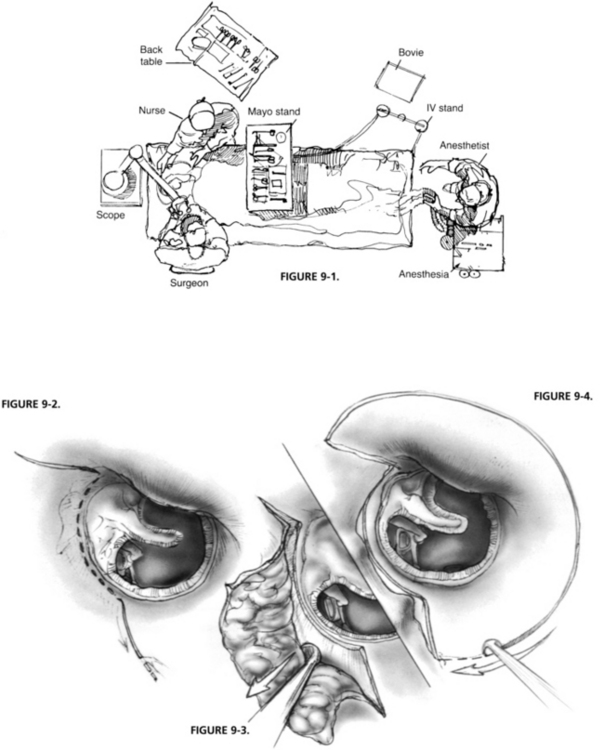
Particular attention should be paid to operating room arrangement (Fig. 9-1). The anesthesiologist is at the patient’s feet, far removed from the operating field, and the scrub nurse is directly across from the surgeon, where the nurse may be of the most assistance. The same arrangement, minus the anesthesiologist, is used for procedures done with the patient under local anesthesia.
SURGICAL TECHNIQUE
The lateral surface grafting technique involves eight steps: (1) transmeatal canal incisions, and elevations of the vascular strip; (2) postauricular exposure, and removal and dehydration of the temporalis fascia; (3) removal of canal skin; (4) enlargement of the ear canal by removal of the anterior (and inferior) canal bulge; (5) de-epithelialization of the tympanic membrane remnant; (6) placement of the rehydrated fascia on the outer surface of the remnant, but under the manubrium; (7) replacement of canal skin; and (8) closure of the postauricular incision and replacement of the vascular strip transmeatally.10
Transmeatal Incisions
Incisions are made along the tympanomastoid and tympanosquamous suture lines, demarcating the vascular strip with a No. 1 (sickle) knife (Fig. 9-2). The vascular strip is the area of the canal skin that covers the superior and posterior portions of the ear canal between these two suture lines. It is easily demarcated from the skin of the remainder of the ear canal because of its thickness, and the fact that it balloons up when local anesthesia is injected into the area. The vascular strip is elevated from the bone, from within outward using a round knife (Fig. 9-3).
A semilunar incision is made in the outer third of the ear canal, using a Beaver knife with a No. 64 blade, connecting the two incisions already made along the border of the vascular strip (Fig. 9-4). The knife blade is angled toward the bone to thin the 1 or 2 mm section of the membranous canal included.



