Tumors of the Oral Cavity and Jaw
Tumors of the jaw may impinge on the oral cavity and alter oral function as well as affect facial appearance.
21-1 Excision of Fibrous Dysplasia
Introduction
Fibrous dysplasia is a benign locally invasive fibro-osseous disorder. In its most common monostotic form, it involves the maxilla more often than the mandible. The lesion usually presents with an obvious deformity of the involved bony structure (Fig. 21.1a).
Indications
Surgery is indicated both to confirm the diagnosis and to sculpt the lesion to restore normal anatomy and function. Radical excision of this lesion is never indicated. Repeat procedures may be required to treat this slow-growing lesion.
Preoperative Evaluation
Computed tomography (CT) scan of the affected bony area is mandatory before surgical intervention.
Operative Technique
1. General anesthesia is administered through a nasal endotracheal tube placed in the uninvolved side. If the lesion involves the maxilla, the usual approach to this area is the gingivobuccal approach as in the Caldwell-Luc procedure.
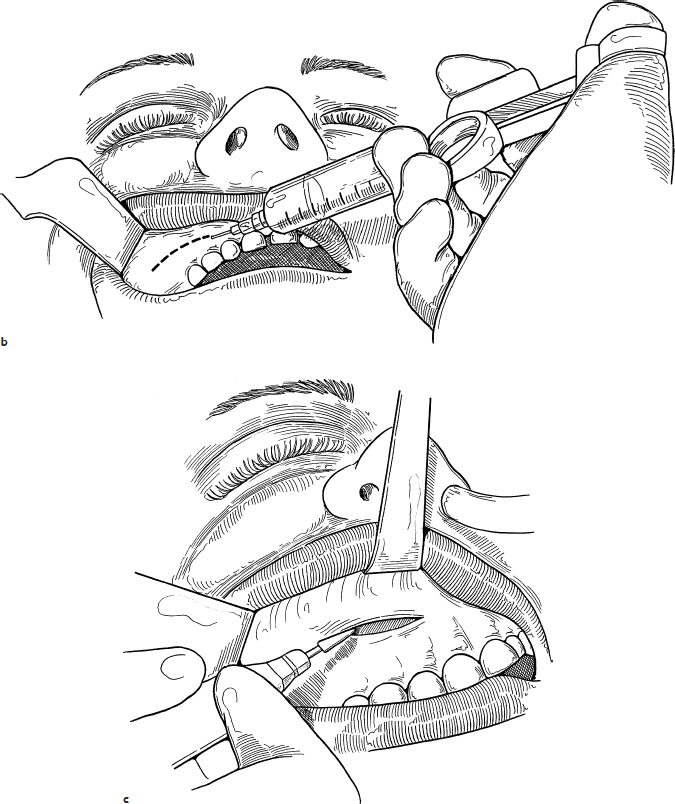
2. One percent lidocaine with 1:100,000 epinephrine is injected into the gingivobuccal sulcus (Fig. 21.1b).
3. An incision in the gingivobuccal sulcus 5 mm above the gum line is made with a no. 15 blade. The incision is carried down to the periosteum of the maxilla with the cutting cautery (Fig. 21.1c).
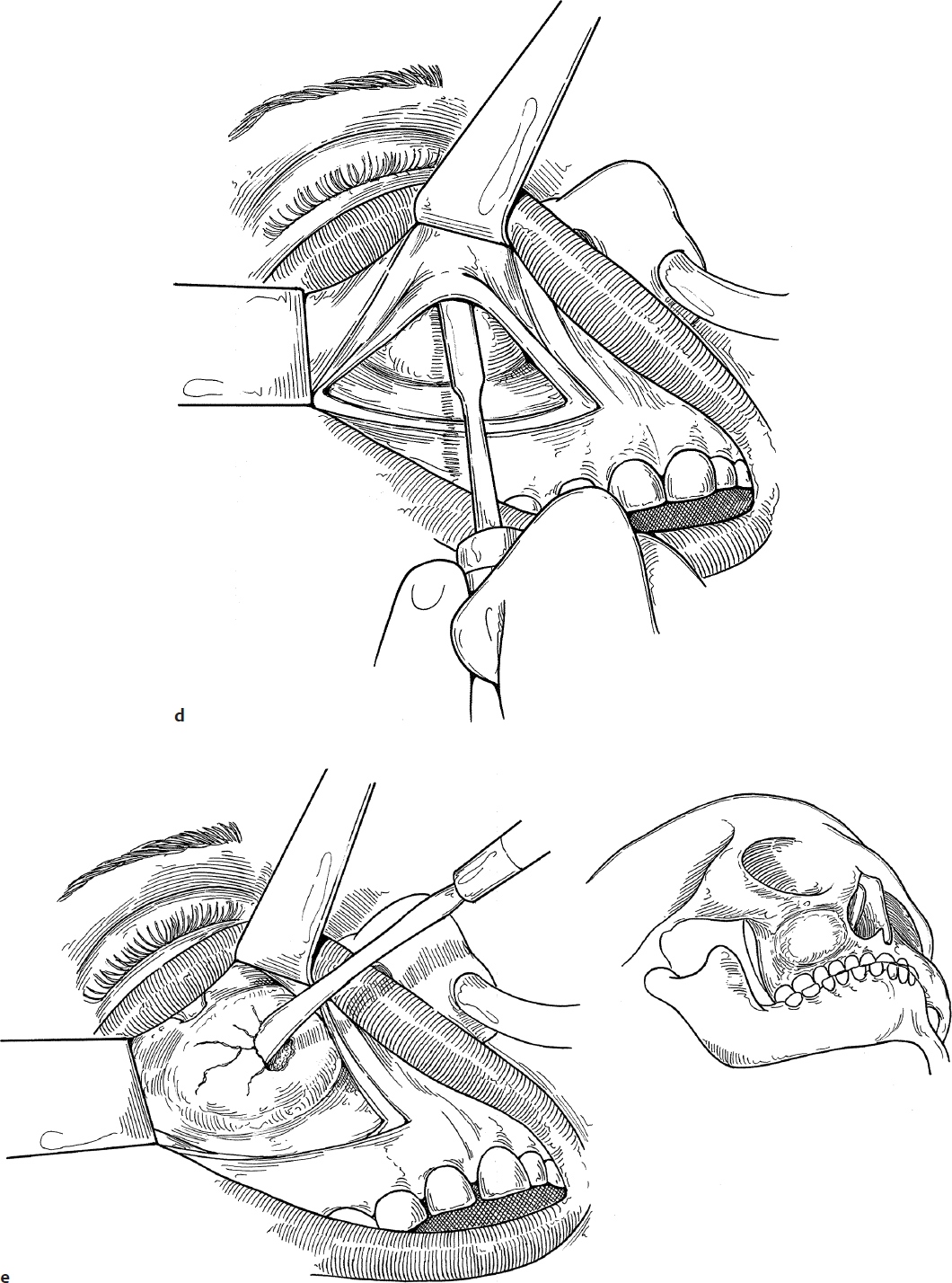
4. A periosteal elevator is used to elevate the soft tissues of the cheek off of the face of the maxilla until the infraorbital nerve is identified (Fig. 21.1d).
5. If there is a thin layer of normal bony cortex, this is cracked and removed with a small curved clamp or elevator (Fig. 21.1e).
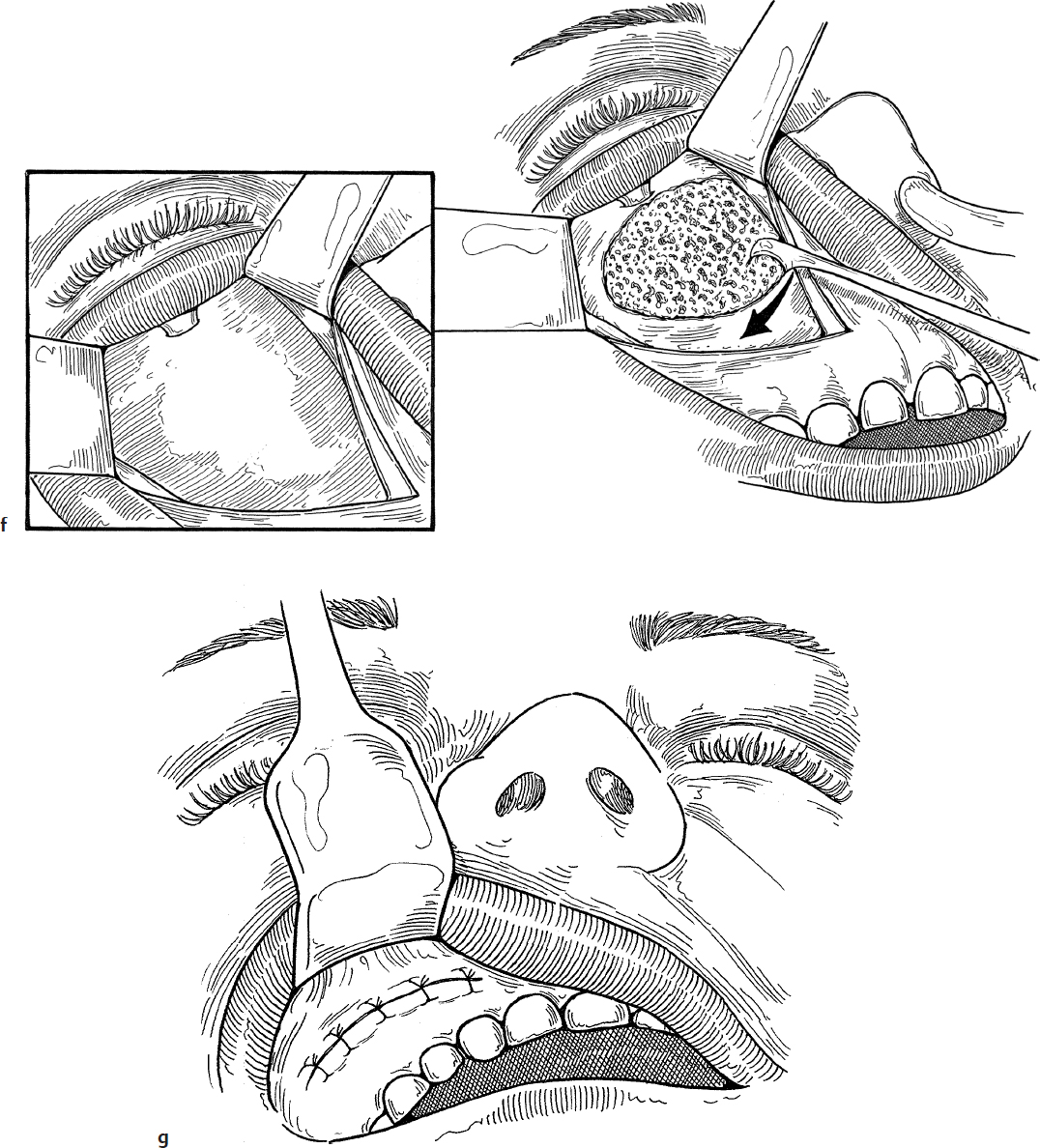
6. The tumor is debulked with a knife or large cup forceps (Takahashi) or curette, depending on its gritty nature. When the desired contour has been obtained, the operation is terminated (Fig. 21.1f). If there is a patent maxillary sinus cavity, patency of the maxillary ostia should be confirmed with nasal endoscopy, and endoscopic antrostomy should be done if needed.
7. The mucosa of the cheek is sutured loosely with interrupted 4-0 chromic sutures. These sutures are left in place until they dissolve on their own (Fig. 21.1g).
Complications
1. Recurrence from incomplete excision
2. Ocular injury
3. Infraorbital nerve injury

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


