The sequelae of trauma to the nose include nasal deformity and nasal obstruction that can have a long-term negative impact on patient quality of life. Successful management of posttraumatic nasal obstruction relies on a detailed history, careful analysis, and accurate diagnosis. Dividing the nose into horizontal thirds assists in preoperative analysis as well as surgical treatment. Adequate treatment of posttraumatic nasal obstruction must address deflection of the bony nasal pyramid, septal deformities (especially caudal or dorsal), turbinate hypertrophy, and incompetence of internal and external nasal valves. Treatment must balance the seemingly disparate goals of re-establishing structure, improving contour and esthetics, as well as restoring the nasal airway.
The nose is considered the most prominent feature of the face. As a result, fractures of the nose and nasal region account for approximately half of all facial fractures. The sequelae of trauma to the nose include nasal deformity and nasal obstruction that can have a long-term negative impact on patient quality of life and thus often require repair. According to Rohrich and Adams, 40% to 42% of patients after nasal trauma have significant septal deformities that require subsequent septorhinoplasty. This article focuses on the treatment of nasal obstruction in the posttraumatic nose. Nasal obstruction following trauma is a complex problem that poses several challenges for the facial plastic surgeon. Successful management of posttraumatic nasal obstruction relies on careful analysis and accurate diagnosis. Treatment of the posttraumatic nose must balance the seemingly disparate goals of re-establishing structure, improving contour and esthetics, and restoring the nasal airway.
Etiology
Trauma to the nose is most often sustained in fights (34%), accidents (28%), and sports (23%). Frontal force causes damage ranging from simple fracture of the nasal bones to severe flattening of the nasal bones and septum. Splaying of the nasal bones with widening of the nasal width may also occur. Lateral force may depress only one nasal bone; however, with sufficient force, both bones may be displaced. In addition, lateral force can cause severe septal displacement, which can further twist or buckle the nose. Septal fragments may overlap, creating further difficulty in reduction. Furthermore, a C-shaped deformity may occur. This defect usually begins under the dorsum of the nose, extends posteriorly and inferiorly through the perpendicular plate of the ethmoid, and ends with an anterior curve in the cartilaginous septum approximately 1 cm above the maxillary crest. Superior-directed force is rare and may cause severe septal fractures and dislocation of the quadrangular cartilage. With the increasing use of air bags in automobiles, a shift in the mechanism of injury and the type of nasal fractures has occurred, resulting in an increase in the incidence of septal injury in nasal fractures without concurrent nasal bone fracture.
Analysis of the posttrauma nose
The cornerstone of a thorough analysis is a detailed history with particular attention to the type, date, and frequency of traumatic events as well as any previous surgeries. Even seemingly minor trauma early in life can produce a delayed marked deformity not manifesting itself until the nose and face grow significantly at puberty. The date of trauma and any past surgeries is important because it may influence the timing of any further surgery that may be required. Although closed reduction of nasal bone fractures may be performed either within the first several hours following injury before the development of significant edema or between 4 to 7 days following the injury after the resolution of facial edema, an open approach is often required if nasal obstruction is to be adequately addressed in addition to nasal deformity. In these cases, a delay of 6 to 12 months after injury is often required to allow fractures to stabilize and wounds to heal before surgical correction of nasal obstruction or deformity. Patients who have sustained multiple traumas or have had previous nasal surgery may not only be more complex but may also lack any usable septal cartilage grafts. As a result, it is important to ask patients about any prior history of nasal surgery or pre-injury septal deviation. In addition, it is critical to ask patients about the existence of any pre-injury/presurgery nasal obstruction, because they may have underlying unrecognized deviation of the septum or untreated allergic rhinitis or other medical conditions.
A thorough examination is crucial to identifying causes of nasal obstruction in the posttraumatic patient before and after topical decongestion. Anterior rhinoscopy is a valuable tool for assessing the patient. In addition, nasal endoscopy can be useful in the evaluation of patients with posttraumatic nasal obstruction. In a study of 96 consecutive patients undergoing rhinoplasty, preoperative endoscopy identified pathology that required additional surgery in 28 patients, including concha bullosa, posterior septal deviation, adenoid hypertrophy, choanal atresia, and intranasal tumor. The physical examination should be carefully performed, starting with inspection of the septal mucosa for inflammation or other mucosal disease. The septum should also be examined for tears, synechiae, and evidence of septal fractures or perforations. The septum should be evaluated for any deviation, particularly high dorsal or caudal deflection. The presence of turbinate hypertrophy should be noted. In addition, careful attention should be paid to patency of the external nasal valve by identifying any vestibular stenosis, tip ptosis, collapse of the lower lateral cartilages, or nasal muscle deficiency. Furthermore, the zones and grade, as described by Most, of any external nasal valve collapse should be noted. Most categorizes external nasal valve collapse into two zones. Zone 1 is the upper lateral cartilage complex, whereas zone 2 is at or below the junction between the upper and lower lateral cartilages. Collapse at these zones is graded as a percentage of airway closure between the lateral nasal wall and the septum; grade 1 is 0% to 33%, grade 2 is 33% to 66%, and grade 3 is 66% to 100%.
The internal nasal valve should be examined for patency by analyzing the nasal valve area including the nasal septum, upper and lower lateral cartilages (in particular, inferomedial displacement of the upper lateral cartilage), adjacent fibrofatty tissue, piriform aperture, head of the inferior turbinate, and floor of the nose. A diagnosis can be made based on direct inspection of valvular support during quiet and forced inspiration without the distortion induced by a nasal speculum. Collapse of the internal nasal valve can be attributed to medialization of the caudal margin of the upper lateral cartilages due to negative pressure created on inspiration through the nose; these patients typically have pinching or medial collapse of the supra-alar region. The Cottle maneuver is often used to assess internal nasal valve competence. In patients with internal valve collapse, there is often improvement in nasal breathing with lateral retraction of the ipsilateral cheek skin. A modified Cottle maneuver can also be performed with a cotton-tip swab placed intranasally to support the internal nasal valve to determine specifically if improvement in nasal airflow results.
Analysis of the posttrauma nose
The cornerstone of a thorough analysis is a detailed history with particular attention to the type, date, and frequency of traumatic events as well as any previous surgeries. Even seemingly minor trauma early in life can produce a delayed marked deformity not manifesting itself until the nose and face grow significantly at puberty. The date of trauma and any past surgeries is important because it may influence the timing of any further surgery that may be required. Although closed reduction of nasal bone fractures may be performed either within the first several hours following injury before the development of significant edema or between 4 to 7 days following the injury after the resolution of facial edema, an open approach is often required if nasal obstruction is to be adequately addressed in addition to nasal deformity. In these cases, a delay of 6 to 12 months after injury is often required to allow fractures to stabilize and wounds to heal before surgical correction of nasal obstruction or deformity. Patients who have sustained multiple traumas or have had previous nasal surgery may not only be more complex but may also lack any usable septal cartilage grafts. As a result, it is important to ask patients about any prior history of nasal surgery or pre-injury septal deviation. In addition, it is critical to ask patients about the existence of any pre-injury/presurgery nasal obstruction, because they may have underlying unrecognized deviation of the septum or untreated allergic rhinitis or other medical conditions.
A thorough examination is crucial to identifying causes of nasal obstruction in the posttraumatic patient before and after topical decongestion. Anterior rhinoscopy is a valuable tool for assessing the patient. In addition, nasal endoscopy can be useful in the evaluation of patients with posttraumatic nasal obstruction. In a study of 96 consecutive patients undergoing rhinoplasty, preoperative endoscopy identified pathology that required additional surgery in 28 patients, including concha bullosa, posterior septal deviation, adenoid hypertrophy, choanal atresia, and intranasal tumor. The physical examination should be carefully performed, starting with inspection of the septal mucosa for inflammation or other mucosal disease. The septum should also be examined for tears, synechiae, and evidence of septal fractures or perforations. The septum should be evaluated for any deviation, particularly high dorsal or caudal deflection. The presence of turbinate hypertrophy should be noted. In addition, careful attention should be paid to patency of the external nasal valve by identifying any vestibular stenosis, tip ptosis, collapse of the lower lateral cartilages, or nasal muscle deficiency. Furthermore, the zones and grade, as described by Most, of any external nasal valve collapse should be noted. Most categorizes external nasal valve collapse into two zones. Zone 1 is the upper lateral cartilage complex, whereas zone 2 is at or below the junction between the upper and lower lateral cartilages. Collapse at these zones is graded as a percentage of airway closure between the lateral nasal wall and the septum; grade 1 is 0% to 33%, grade 2 is 33% to 66%, and grade 3 is 66% to 100%.
The internal nasal valve should be examined for patency by analyzing the nasal valve area including the nasal septum, upper and lower lateral cartilages (in particular, inferomedial displacement of the upper lateral cartilage), adjacent fibrofatty tissue, piriform aperture, head of the inferior turbinate, and floor of the nose. A diagnosis can be made based on direct inspection of valvular support during quiet and forced inspiration without the distortion induced by a nasal speculum. Collapse of the internal nasal valve can be attributed to medialization of the caudal margin of the upper lateral cartilages due to negative pressure created on inspiration through the nose; these patients typically have pinching or medial collapse of the supra-alar region. The Cottle maneuver is often used to assess internal nasal valve competence. In patients with internal valve collapse, there is often improvement in nasal breathing with lateral retraction of the ipsilateral cheek skin. A modified Cottle maneuver can also be performed with a cotton-tip swab placed intranasally to support the internal nasal valve to determine specifically if improvement in nasal airflow results.
Treatment of posttraumatic nasal obstruction
Careful planning is critical to successful treatment of posttraumatic nasal obstruction. Dividing the nose into horizontal thirds assists in preoperative analysis as well as surgical treatment to re-establish structure, improve contour and esthetics, and restore the nasal airway.
Upper Third of Nose
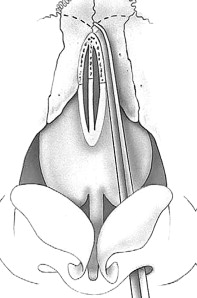
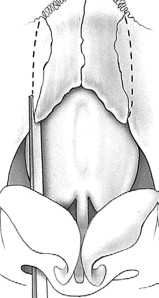
The upper third of the nose consists of the nasal bones, nasal process of the frontal bone, and frontal process of the maxilla. Osteotomies are often employed in rhinoplasty to close an open nasal vault, to narrow the nasal dorsum, or to straighten a deviation in the nasal dorsum. Lateral osteotomies are performed in a high-low-high fashion, starting at the anterior end of the inferior turbinate perpendicular to the edge of the piriform aperture and curved anteriorly and superiorly in the nasofacial groove toward the medial canthus ( Fig. 1 ). Next, either a superior back fracture, accomplished by turning the osteotome and applying digital pressure, or a superior percutaneous transverse osteotomy is performed. Medial osteotomies are performed between the nasal bones and the septum and angulated superiorly to join the superior osteotomy or back-fractured site ( Fig. 2 ). When one sidewall is significantly longer than the other, intermediate osteotomies may also be used. Intermediate osteotomies are performed prior with their path parallel to lateral osteotomies, because the former are difficult once the nasal bone is mobilized ( Fig. 3 ). In the context of the posttraumatic nose, osteotomies can be used to expand the nasal airway as well as restore the nasal contour of the twisted or deviated nose. When used to address the nasal airway, lateral push-out osteotomies followed by medial osteotomies are used to accommodate a spreader graft and widen the airway. When used to correct deflection of the bony vault, sequential osteotomies are performed from lateral to medial starting on the concave side, often likened to turning the pages of an open book ( Fig. 4 ). Using this technique, the concave side is first mobilized to create sufficient space to reposition the deviated structures.

Middle Third of Nose
Treatment of deformities of the middle third is critical to improving the nasal airway. The middle third of the nose includes the upper lateral cartilages, septum, and piriform aperture. Septal pathology may involve cartilage, bone, or both. The septum may be thickened, twisted, scarred, deflected off the maxillary crest, have spurs, or be affected by a combination of these problems. Deviation of the septum secondary to septal fracture or pre-existing septal deflection exacerbated by trauma can often be treated with septoplasty. Convexity or concavity of the septal cartilage can be treated by scoring, crushing, or removal with or without replacement of crushed cartilage between the mucopericondrial flaps. High septal or dorsal deflections may be addressed via an external approach. In addition, inferior turbinate hypertrophy should also be addressed in the treatment of posttraumatic nasal obstruction. Patients with septal deviation have pre-existing turbinate hypertrophy; the inferior turbinate contralateral to the direction of septal deflection is the larger turbinate. Often, turbinate reduction is necessary to mobilize the septum back to the midline. There are many different techniques of turbinate reduction, including monopolar or bipolar cautery, radiofrequency ablation, submucous resection of bone and soft tissue, and partial inferior turbinectomy. Following reduction, the turbinate is then out-fractured laterally.
Internal valve insufficiency is caused variably by a narrow angle between the upper lateral cartilage and the septum, deviation of the septum, or enlargement of the anterior portion of the inferior turbinate. Treatment of internal valve insufficiency is critical to improve nasal obstruction in the posttraumatic nose. One must counsel patients that many of the techniques used to address nasal obstruction caused by abnormalities of the internal valve may change the appearance of the nose by widening it. Several techniques have been used to correct internal nasal valve collapse; these techniques are focused on repositioning of the upper lateral cartilage or the addition of structural grafts to support the lateral wall of the nose. The traditional technique used to address internal nasal valve collapse has been the placement of spreader grafts via an endonasal or external approach. These grafts are designed to lateralize the upper lateral cartilage by the width of the graft, thereby increasing the cross-sectional area of the nasal valve. Septal, conchal, costal, or cadaveric cartilage, bone, or even Medpor may be used as potential sources for spreader grafts. The grafts, typically 1 to 2 mm thick spanning the length of the upper lateral cartilage, are placed in a submucosal pocket between the septum and upper lateral cartilage and fixed in place with one or two horizontal mattress sutures ( Fig. 5 ). Studies have shown that spreader grafts are effective in treating nasal obstruction due to internal nasal valve narrowing. A variation of this technique involves use of the upper lateral cartilages as autospreaders. After dorsal hump reduction, spreader grafts are often required to maintain the internal nasal valve angle. The bony and cartilaginous hump is removed, taking care to preserve the upper lateral cartilages and mucopericondrium. The overprojecting portion of the upper lateral cartilages is then rotated medially to lie between the septum and the medial edge of the upper lateral cartilages ( Fig. 6 ). The new dorsal edges of the upper lateral cartilages are then sutured to the rotated autospreader cartilages and secured along the septum.
Alternative techniques in the repair of a narrowed internal nasal valve include dorsal onlay grafts, flaring sutures, and alar batten grafts. Dorsal onlay grafts employ a single piece of cartilage placed over the nose, from bony nasal dorsum to the anterior septal angle, and sutured laterally to each upper lateral cartilage to open the nasal valve. Dorsal onlay grafts are often used to correct severe middle nasal vault deformity and resultant airway problems, particularly in saddle nose deformities. Constantian and Clardy evaluated and compared the efficacy of spreader grafts and dorsal grafts in supporting the internal valves and noted that they were equally effective. In addition, placement of a flaring suture is a method of improving the internal nasal valve angle directly and usually follows the placement of spreader grafts. It consists of a mattress suture placed through each upper lateral cartilage and over the dorsum. As the suture is tightened, both upper lateral cartilages are pulled dorsally, resulting in a “flaring” action which directly widens the internal nasal valve angle.
The use of alar batten grafts is not only effective for the correction of internal valve collapse but also effective in treating external nasal valve collapse. The primary purpose of batten grafts is to reinforce areas of the lateral nasal wall or the alar lobule that collapse secondary to the negative force associated with inspiration. They are placed into a precise pocket at the point of maximal lateral wall collapse, most often using either septal or conchal cartilage as sources of graft materials. For internal nasal valve collapse, battens are typically placed in a pocket at the site of supra-alar collapse and are usually near the caudal margin of the upper lateral cartilage ( Fig. 7 ). When external nasal valve collapse is treated, the grafts are typically placed into a pocket caudal to the lateral crura. Batten grafts are wider laterally toward the piriform aperture, to provide maximal structural support, and thin with beveled edges, especially along the medial aspect of the graft, to minimize cosmetic distortion. The support and stabilization of the lateral nasal wall increases the internal diameter of the nasal airway, thereby increasing dynamic nasal airflow. In a 46-patient review, Toriumi and colleagues concluded that alar batten grafts are effective for long-term correction of internal and external nasal valve collapse in patients who do not have intranasal scarring in the region of the nasal valve, loss of vestibular skin, or excessive narrowing at the piriform aperture.



