Leprosy is a chronic granulomatous infection of the skin and peripheral nerves that often leads to gross deformation of the nasal skeleton and subsequent formation of a saddle-nose deformity. Reconstruction of the nose following Mycobacterium leprae infection has challenged surgeons for centuries. As a result, a number of different techniques have been attempted with varying outcomes. This article describes the case and surgical treatment of a 37-year old female who presented with a subtotal nasoseptal perforation and saddle-nose deformity secondary to previous infection with leprosy. Reconstruction was achieved via an open septorhinoplasty approach using autologous costal cartilage grafts, yielding a successful postoperative result.
Leprosy is a chronic granulomatous infection of the soft tissue of the skin and peripheral nerves that has plagued industrialized human populations worldwide for thousands of years. Leprosy remains a commonly occurring disease in some countries, with over 219,000 cases reported and a prevalence of more than one case per 10,000 people. Unfortunately, despite medications that can effectively treat leprosy, it remains a difficult disease to detect, and diagnosis often occurs after the onset of several specific deformities. One of the most common manifestations of leprosy is the destruction of nasal cartilage. Interestingly, this disease universally preserves the skin, mucosa, and lower lateral cartilages of the nose.
Believed to have originated in the Indian subcontinent, the disease traversed the globe from Europe to Africa, along with the Far East and South America. However, since the description of the causative etiologic agent, Mycobacterium leprae , in 1873 by Gerhard HA Hansen, the disease has become concentrated mostly in resource-poor countries within tropical climate zones. Currently, 83% of recorded cases of the disease are found in only six countries: India, Brazil, Burma, Indonesia, Madagascar, and Nepal. Because of the large immigrant influx into major metropolitan cities within the United States, coupled with leprosy patients frequently presenting with signs and symptoms of the disease long after leaving an endemic region, it is important that clinicians in the United States be able to diagnose and treat manifestations of this disease.
Although there are numerous functional and cosmetic consequences secondary to lepromatous disease, perhaps none is more distressing or socially stigmatized than the development of a saddle-nose deformity. Inhalation of the mycobacterium allows for infiltration of the nasal mucosa and subsequent destruction of the bony and cartilaginous skeleton along with the mucosal lining. This process results in extensive remodeling of the nasal framework and significant ensuing deformities. Surgeons have proposed a variety of reconstructive techniques, which include nasolabial turnover flaps, post-nasal skin grafts, silicone rubber implants and other external prostheses, and most recently, autologous auricular and/or costal cartilage grafts. This article presents a case of severe saddle-nose deformity secondary to prior infection with Mycobacterium leprae (leprosy), and successful reconstruction with autologous costal cartilage grafts.
Case report
A 37-year old female born in the Dominican Republic, and a recent immigrant to the United States, presented with a complaint of complete nasal collapse. Her pertinent history began 7 years previously at age 30, when she sought medical attention from a dermatologist for multiple skin lesions developing on her upper extremities and trunk. A diagnosis of leprosy was made based on histologic evidence, and the patient was treated for several months with “multiple antibiotics.” Beginning in her mid-30s, the patient began to note progressive changes in the structure of her nose, along with significant nasal obstruction. Gradually, she noticed her entire nose “collapse.” Family members and friends had difficulty recognizing her. The patient does not report a history of other family members contracting or having been treated for leprosy in the past. The leprosy has been “quiescent” for a period of 2 years since her last treatments, the details of which she did not recall.
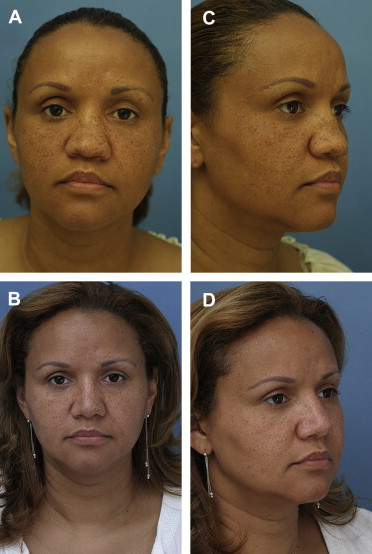
Physical examination demonstrated a woman with a severe saddle nose deformity and total nasal septal perforation. The patient had decreased tip support and recoil, which resulted in a bulbous, underprojected nasal tip. Aside from significant middle vault collapse, she also demonstrated deficient premaxillary projection ( Fig. 1 ).
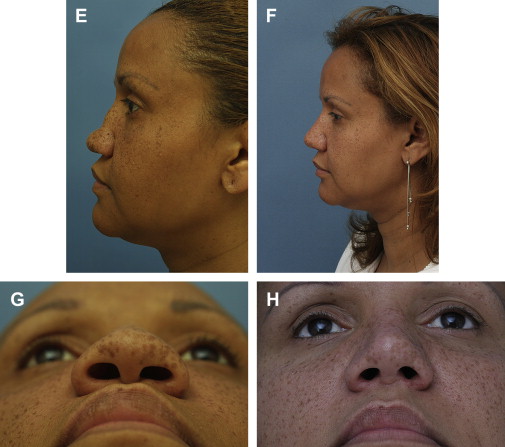
A nasal reconstruction was performed via an open rhinoplasty approach. Costal cartilage from two ribs—specifically the left seventh and eighth ribs—were harvested to repair her nose. Support of the nasal base was achieved with an extended columellar strut, carved from costal cartilage. The strut was carved to help project the nasal tip and augment the columella and premaxilla. The strut was not integrated with the residual septum ( Fig. 2 ) Two interrupted permanent sutures were placed through the periosteum along the nasal spine to stabilize the graft ( Figs. 3 and 4 ). In an effort to augment the premaxilla, several small pieces of costal cartilage (2 mm × 2 mm × 2 mm) were placed in a precisely made intranasal pocket and closed with 4-0 chromic gut sutures (Ethicon, Somerville, New Jersey).
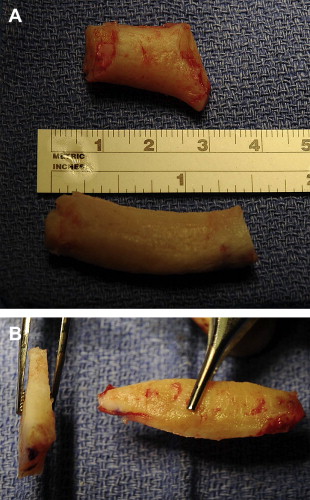
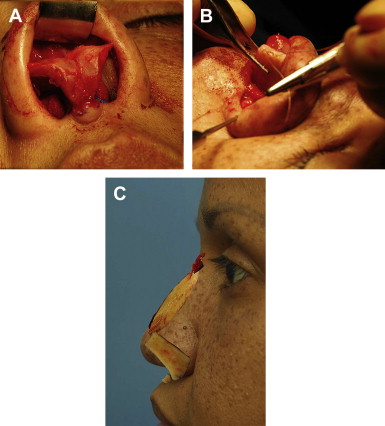
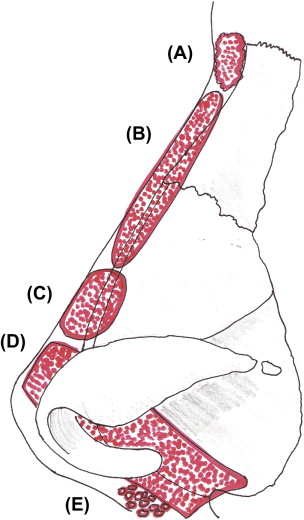
A mild boney dorsal reduction was undertaken with a rasping technique to allow for a smooth platform for nasal dorsum augmentation. A thinly-sculpted dorsal onlay graft was placed over the nasal bones and upper lateral cartilages. The graft was carved from the soft central core of costal cartilage in an effort to mitigate the risk of cartilaginous warping. Furthermore, a moderately-crushed cartilagenous graft was placed over the middle third. Finally, the radix was augmented with remaining costal perichondrium (see Fig. 4 ).
Leprosy epidemiology
The pathology of nasal skeleton collapse in leprosy begins with nasal septal mucosal edema and subsequent destruction following infiltration with Mycobacterium leprae , an inhaled pathogen. The majority of patients with nasal collapse have long-standing disease. Initially, the damage is microscopic; however, as the disease progresses, the destruction becomes visible on gross examination. After the nasal septal mucosa is destroyed, the underlying quadrangular cartilage is exposed leading to secondary bacterial infection. Alternatively, exposure necrosis may result secondary to vascular ischemia, with the loss of the perichondrial blood supply. The end result is septal perforation. Those structures covered by respiratory mucosa on both surfaces, including the nasal septum, nasal spine of the maxilla, and the turbinates, are most prone to destruction. As the nasal spine is resorbed, the classic saddle-nose deformity can develop, accompanied by an acute nasolabial angle and a deficiency of columellar show. Progression of the disease often occurs with partial or complete destruction of the nasal bones with resultant flattening of the nasal bridge. In rare cases, scar tissue retraction can lead to virtual elimination of the nasal vestibule, thereby causing significant functional deficits. Fortunately, it is exceedingly rare for the nasal skin–soft tissue envelope to be affected by the disease.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


