17 Treatment of Injuries of the Skull Base Any skull base defect with detection of cerebrospinal fluid leakage demands reconstruction of the bony skull base that provides mechanically stable support for the cranial contents and watertight closure of the endocranium. Table 6.4 lists absolute and relative surgical indications. Surgical access is determined by the localization of the injury of the skull base (Table 17.1). The chosen approach should always ensure the potential for simultaneous management of midfacial injuries without the need for an additional incision. A skin incision is made from ear-to-ear, placed bilaterally preauricular over the temporalis muscle attachment, running 2 cm behind the hairline to a point inferior to the tragus (Fig. 17.1). After dissecting the subcutaneous layer, the periosteum is incised. Subperiosteal dissection minimizes the extent of postoperative swelling. Dissection proceeds beneath the periosteum to the temporal fossa. To avoid injury of superficial nerve branches of the facial nerve, care must be taken with further incision to strictly dissect against the temporal fascia or in the subfascial plane. The supraorbital nerve is exposed on both sides within its bony canal; then the orbits are exposed. In the course of dissection, the entire central midface can be exposed down to the lacrimal sac. If the incision is continued bilaterally to inferior of the tragus, dissection allows visualization of the cartilaginous nasal skeleton. In fractures of the anterior wall of the frontal sinus, primary reconstruction of any fragments should be attempted if they are still connected. Removal of fragments is absolutely contraindicated. Reconstructed portions of the anterior wall of the frontal sinus can be elevated with osteosynthesis plating. In the absence of fracture, the anterior wall of the frontal sinus is opened using a mini saw blade to form an osteoplastic flap.
 Checklist Injuries of the Skull Base, Chapter 3, p. 16.
Checklist Injuries of the Skull Base, Chapter 3, p. 16.
 Antibiotic Therapy, Chapter 24, p. 210.
Antibiotic Therapy, Chapter 24, p. 210.
 Diagnosing Injuries of the Skull Base, Chapter 6, p. 45.
Diagnosing Injuries of the Skull Base, Chapter 6, p. 45.
Indications
Approaches
Ear-to-Ear Scalp Incision, Bicoronal Incision
Type | Localization | Approaches |
I | Posterior wall of frontal sinus | Bicoronal incision, frontoorbital approach based on Killian |
II | Anterior ethmoid, cribriform plate | Bicoronal incision, frontoorbital approach based on Killian |
III | Posterior ethmoid | Endonasal |
IV | Sphenoid sinus | Endonasal |
V | Orbital roof | Bicoronal incision, eyebrow incision |
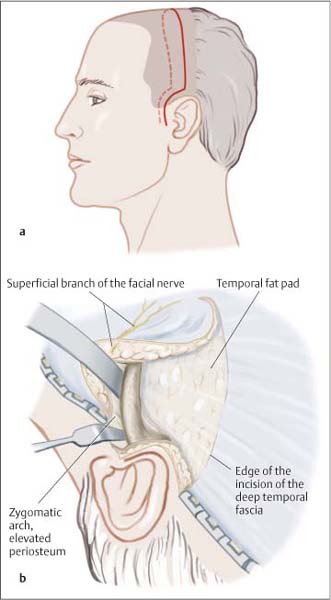
Fig. 17.1 Schematic illustration of the bicoronal incision.
a Incision carried to anterior to the tragus.
b To preserve the facial nerve, dissection beneath the temporal fascia to the zygomatic arch.
Frontoorbital Approach
An arc-shaped incision is made in the medial portion of the eyebrows, travelling to caudal between the nasal dorsum and medial canthus, and ending in the infraorbital ridge (Fig. 17.2). The incision can also be combined with a primary Z-plasty at the canthus. The skin, subcutaneous tissues, and periosteum are dissected at the same time, maintaining a strict vertical position of the scalpel all the way to the underlying bone. Hemorrhage in the distribution area of the supraorbital artery must be precisely controlled. Preservation of the supraorbital nerve during dissection is absolutely imperative.

Fig. 17.2 Exposure of the posterior wall of the frontal sinus using a frontoorbital approach. The defect in the skull base is indicated with a star.
After placing the skin incision, the soft tissues and periosteum are stripped from the floor of the frontal sinus and the lateral margin of the nasal bone. Attention must be paid to strict subperiosteal dissection in the areas of attachment of the medial canthal ligament and near the trochlea. The floor of the frontal sinus and the sphenoid can then be opened with osteoplastic or osteoclastic techniques. Care must be taken to close the surgical wound with precise, multi-layered reconstruction, ensuring periosteal adaptation.
Endonasal Approach
Transnasal microscopic surgery and endoscopic surgery are among the least invasive techniques. Defects in the posterior ethmoid region and sphenoid sinus can be covered without difficulty and necessary drainage of the paranasal sinuses can also be performed during the intervention.
Surgical Technique
Principles of Dural Repair
Prior to reducing midface fractures, herniated brain tissue must always be mobilized from the fracture gap.
Contused areas are suctioned, taking care to protect the brain tissue with an appropriate cotton strip. Only after reduction and fixation of the midface can definitive management of the skull base injury proceed.
The goal of dural repair is watertight closure of the defect. Various methods are used (Fig. 17.3a):
 Intradural management, overlay: inserting a graft over the defect between the dura mater and brain.
Intradural management, overlay: inserting a graft over the defect between the dura mater and brain.
 Extradural management, underlay: interposing a graft between bone and dura, with the graft acting as a splint for natural closure of the dura.
Extradural management, underlay: interposing a graft between bone and dura, with the graft acting as a splint for natural closure of the dura.
 Sandwich method: covering the dural defect from the paranasal sinus. This can also be used as a complementary measure.
Sandwich method: covering the dural defect from the paranasal sinus. This can also be used as a complementary measure.
 Graft fixation is with fibrin adhesive.
Graft fixation is with fibrin adhesive.
 Cranial or cerebrospinal fluid pressure jeopardizes repair. Risk can be minimized by decreasing cranial pressure (cerebrospinal fluid drainage), the choice of graft (cartilage, cement), and supporting repair with packing.
Cranial or cerebrospinal fluid pressure jeopardizes repair. Risk can be minimized by decreasing cranial pressure (cerebrospinal fluid drainage), the choice of graft (cartilage, cement), and supporting repair with packing.
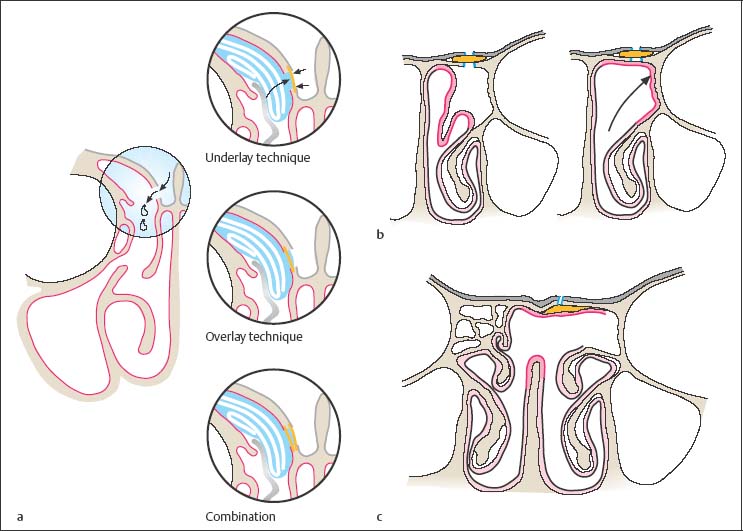
Fig. 17.3 Techniques for covering skull base defects.
a Various techniques for dural repair (from H. Stammberger: Endoscopic diagnostic of the paranasal sinus and the frontal skull base, Storz, Tuttlingen).
b Covering the bony defect with portions from the middle turbinate after grafting using the underlay technique, e. g., in the middle region of the sphenoid bone (region II + III).
c Repair of the bony defect with septal mucosa after overlay grafting.
Frontal Sinus
The coronal incision is the preferred approach for extensive defects, large frontal sinuses, or midfacial fractures.
After osteoplastic removal of the anterior wall of the frontal sinus the bony defect is exposed using a diamond burr. Care must be taken to establish visualization of the full extent of dural injury.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


