Traumatic Cataracts in Children
M. Edward Wilson
Rupal H. Trivedi
Suresh K. Pandey
Ocular trauma is a leading cause of unilateral blindness. Children are particularly vulnerable to ocular injury, especially sports-related ocular injury. Prevention of eye injuries is of utmost importance and is the team responsibility of parents, teachers, coaches, ophthalmologists, pediatricians, and optometrists. The American Academy of Pediatrics and the American Academy of Ophthalmology have published a joint statement recommending types of protective lenses and frames for specific sports.1
CLASSIFICATION OF OCULAR TRAUMA
The Ocular Trauma Classification Group has designed a standardized system for reporting mechanical injury associated with open- and closed-globe trauma. The system is based on the injury type, grade (based on visual acuity), zone, and presence or absence of an afferent pupillary defect.2,3 We provide a short summary of the reporting system below. However, interested readers are referred to the detailed description published by Kuhn2 and Pieramici3 and to the American Society of Ocular Trauma Web site (http://www.asotonline.org).
Closed-Globe Injury
A closed-globe injury is when the eye wall (sclera and cornea) does not have a full-thickness wound. Mechanisms of injury include (1) contusion (blunt force), (2) superficial foreign body, (3) partial-thickness sharp force (lamellar laceration), or (4) a combination of the above.
Open-Globe Injury
An open-globe injury is when the eye wall has a full-thickness wound. These injuries and the mechanisms of injury are further subdivided as outlined below:
Rupture. Full-thickness wound of the eye wall caused by a blunt object. The impact results in a momentary increase in intraocular pressure (IOP) and an inside-out injury mechanism.
Laceration. Full-thickness corneal and/or scleral wound caused by a sharp object. This is an outside-in injury mechanism.
Penetrating injury. Single full-thickness laceration of the eye wall usually caused by a sharp object, with no exit wound.
Intraocular foreign body (IOFB). Retained foreign object(s) causing an entrance laceration(s).
Perforating injury. Two full-thickness lacerations are present with an entrance and exit wound caused by the same agent.
OCULAR TRAUMA AND CATARACT
The crystalline lens may be involved in any case of ocular trauma. Traumatic cataract may be an immediate, early, or late sequel of any ocular trauma. Trauma has been reported to be responsible for up to 29% of all childhood cataracts.4 At the Storm Eye Institute, our database includes more than 100 cases of traumatic cataract. We analyzed 47 consecutive eyes of 47 children operated for traumatic cataract.5 These consecutive trauma cases represented 10.5% of the cataracts we operated during that time interval. Commonly implicated objects leading to the traumatic event include knives, BB guns, firecrackers, sticks, thorns, rocks, pencils, arrows, airbags, paintballs, and toys.
Blunt trauma is responsible for coup and countercoup ocular injury.6 Coup is the mechanism of direct impact. It is responsible for the Vossius ring (imprinted iris pigment) sometimes found on the anterior lens capsule following blunt injury. Countercoup refers to distant injury caused by shockwaves traveling along the line of concussion. When the anterior surface of the eye is struck bluntly, there is a rapid anterior-posterior shortening accompanied by equatorial expansion. This equatorial stretching can disrupt the lens capsule, zonule, or both. Combinations of coup, countercoup, and equatorial expansion are responsible for the formation of traumatic cataracts following blunt ocular injury. Penetrating trauma that directly compromises the lens capsule often leads to
cortical opacification at the site of injury. If the rent is sufficiently large, the entire lens rapidly opacifies. When the capsular rent is small, however, the capsule may seal, and the cortical cataract may remain localized.
cortical opacification at the site of injury. If the rent is sufficiently large, the entire lens rapidly opacifies. When the capsular rent is small, however, the capsule may seal, and the cortical cataract may remain localized.
Cataracts caused by blunt trauma classically form stellate or rosette-shaped posterior axial opacities that may be stable or progressive. At times, an anterior capsular scar (white fibrous capsule) can be seen at the sight of direct impact, especially in children whose eyes are more elastic than those of adults. The pupillary sphincter also often shows multiple small ruptures from blunt trauma, and these may cause a traumatic mydriasis even when the pupil shape is relatively normal.
In penetrating trauma, disruption of the lens capsule often occurs leading to cortical opacification. These cataracts may remain focal if small or may progress rapidly to total cortical opacification. Anterior and/or posterior capsule defect, intralenticular foreign body, partial/total zonular loss, dislocation, and lens subluxation are often found in combination with traumatic cataract. Other associated complications include glaucoma (phacolytic, phacomorphic, pupillary block, and angle recession), phacoanaphylactic uveitis, retinal detachment, choroidal rupture, hyphema, retrobulbar hemorrhage, traumatic optic neuropathy, and globe rupture. Anterior capsule rupture (with flocculent lens matter in the anterior chamber) is usually well tolerated in children. Although an increased IOP and/or lens-induced uveitis (e.g., phacoanaphylactic and phacotoxic endophthalmitis) are known complications of lens rupture, these rarely occur in children. We often cautiously wait 2 to 3 weeks for the eye to heal from the traumatic event before proceeding with cataract surgery (Fig. 35.1), even when flocculent material from lens rupture is seen in the anterior chamber. Outcome of cataract surgery is better when the traumatic iritis and hyphema have subsided.
In the setting of traumatic cataract, the ophthalmologist must first “take a step back” and examine other ocular injuries in detail.7 The cataract surgeon should be suspicious of injury to other ocular structures. Management depends on the degree and type of injury. Localized traumatic cataracts (especially if not in the visual axis) may be managed conservatively, while more significant lens opacities generally require cataract extraction. Similarly, capsular perforation may be managed with observation if small and not centrally located. Frequently, such injuries will develop only very localized opacification of the underlying cortex, without progression to generalized cataracts.
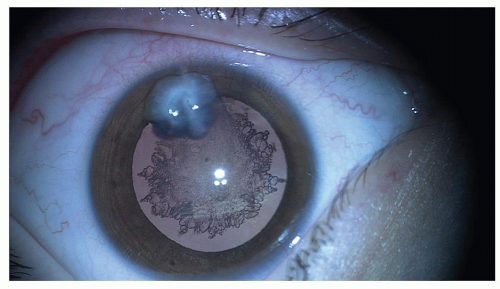 Figure 35.1. A 6-year-old child with traumatic cataract. History of corneal laceration by pencil 2 months ago. |
The initial patient evaluation is one of the most important critical steps in the management of traumatic cataract. Data gathered during this examination, to a large extent, direct further investigations and establish immediate priorities. One of the most important aspects of this first examination is the description of the exact circumstances of the injury. This facilitates the development of risk estimates for occult injuries, such as IOFB, chemical exposure, and posterior rupture of the globe.
Examination
Before Dilation
Best-corrected visual acuity (BCVA).
Fixation preference.
Pupillary reflex: The presence of an afferent pupillary defect may be indicative of traumatic optic neuropathy.
IOP (if there is no evidence of ocular rupture).
Iris: The clinical evaluation should also include a careful predilation examination of the iris for transillumination defects or tears in the pupillary sphincter. If present, it should be documented, and following dilation, the underlying lens surface should also be inspected for an anterior capsular defect that indicates a penetrating injury or IOFB.
Zonule: Although detection of zonular loss is not always possible prior to pupil dilation, suggestive findings include irido- or phacodonesis, an increase in myopic refractive error, abnormal peripheral lens curvature in one or more quadrants, an abnormal light reflex on retinoscopy, a visible lens equator, or vitreous in the anterior chamber.
After Dilation
Slit-lamp examination (after pupillary dilation) is recommended if feasible. The slit-lamp examination helps to identity and document the type of cataract, position and stability of the lens, integrity of the lens capsule, and status of the anterior segment. When slit-lamp examination is not possible in the awake state, it can be done using a portable instrument in the operating room in conjunction with the examination using the operating microscope.
A posterior segment examination, including examination of the retinal periphery, should be carried out in detail if the view through the lens allows. Otherwise B-scan ultrasonography is advisable in all eyes preoperatively.
Gonioscopy may be helpful for evaluating angle structures and for recognizing vitreous at the lens equator or areas of loss of zonular support.
If intraocular lens (IOL) implantation is planned, all eyes need to have keratometry and immersion A-scan ultrasound for globe axial length measurement. Even when corneal scarring is present, keratometry of the injured eye should be attempted. Changes in corneal curvature as the result of an injury will change the IOL power needed to achieve the refractive goal. At times, the keratometry readings of the fellow eye are used, but this can compromise the accuracy of the postoperative refraction in relation to the postoperative goal.
A guarded prognosis for anatomical and functional outcome is to be thoroughly explained to the patient and the patient’s relatives. The full extent of the eye injuries is not always known prior to cataract surgery. The patient and relative must understand that IOL implantation is not always possible at the initial surgery. It is also important to explain about the possible need for additional surgeries depending on the type of injury (retinal detachment, keratoplasty for dense corneal scar obstructing visual axis, etc.). The use of an IOL in traumatic cataracts is well accepted (Fig. 35.2A and B). It offers a constant, maintenance-free optical correction and, as such, helps in the prevention of amblyopia. Malplacement of the IOL is more common in traumatic cataracts since damage to the capsular bag, zonules, and iris may predispose to decentration and pupil capture. In addition, contact lens wear may be helpful after ocular trauma to help compensate for an irregular corneal curvature caused by a healed corneal wound. However, children often have difficulty wearing these lenses due to discomfort and poor motivation to wear the lens.
With this background, we now describe some of our experience with IOL implantation in eyes with traumatic cataract at Storm Eye Institute. Then, we discuss some of the relevant issues related to pediatric traumatic cataracts.8,9,10,11,12,13,14,15,16 These include (1) timing of surgery for pediatric traumatic cataracts, (2) cataract surgery and IOL implantation, (3) postoperative complications, and (4) visual results.
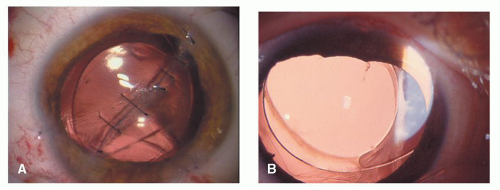 Figure 35.2. A: A 7-year-old boy presented with a history of trauma with knife. A heparin-surface-modified (Pharmacia 722C) IOL implanted. B: Two-month postoperative photo in a 14-year-old child. |
Analyses of Eyes Operated on for Traumatic Cataracts at Storm Eye Institute
We analyzed 23 consecutive eyes with traumatic cataract.5 Ages at IOL implantation ranged from 3.5 to 13.8 years (mean, 6.9 ± 2.5 years). Only 5 (21.0%) of the total 23 patients were females. All 23 children had unilateral cataracts. Nine eyes (39.0%) suffered blunt injury and 14 (60.0%) had penetrating injuries with prior repair of a corneoscleral laceration. The injury preceded cataract surgery by 1 day to 7 years. Nineteen patients (82.6%) had cataract surgery within 3 months of the initial injury. Treatment prior to IOL implantation included repair of the corneoscleral laceration secondary to penetrating trauma in 13 children (56.5%) and repair of a limbal rupture after blunt injury in 1 case (4.3%). Six patients (26.0%) had undergone amblyopia therapy prior to cataract surgery. Preoperative BCVA ranged from 20/40 to possible light perception.
An IOL implantation was performed at the time of cataract removal in 20 eyes (87.0%), while 3 eyes (13.0%) underwent secondary IOL implantation. Two of these patients (who underwent secondary IOL implantation) demonstrated amblyopia preoperatively (vision, 20/50 and 20/100 with poor fusion or strabismus). Traumatic cataracts were noted to be “dense,” “white,” or “total” in 14 of the patients (60.0%), “cortical” in 4 (17.3%), and posterior subcapsular in 2 patients (8.6%), who underwent a primary IOL implantation procedure. Ten patients (43.4%) had an anterior capsule rupture due to the ocular injury noted at presentation or at the time of surgery (Fig. 35.3A and B




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
