9 Trauma
Indications
• Foreign bodies
• Impalement and gun shot, open injury
• Midfacial and orbital fracture
• Skull base fracture, dural defects
• Complications of endoscopic sinus surgery
Principles
A great variety of injuries of the midface and anterior skull base can be managed by direct inspection and repair via minimally invasive endoscopic or microscopic approaches, which have been described in the preceding chapters. Many lesions of traumatic origin, on the other hand, require an external or a combined external–transnasal access. Their optimal selection depends on a precise preoperative diagnosis by imaging and clinicochemical tests, and on the individual precepts and experience of the rhinosurgeon, who also must reconsider possible cooperation with maxillofacial surgeons and neurosurgeons for the prospect of completely natural reconstruction. Such interdisciplinary collaboration is especially valuable in cases of severe skull–brain trauma. Intimate knowledge of the anatomical structures and of the immanent biological forces of spontaneous healing–but also of possible complications–is a precondition for adequate planning of the least aggressive procedure that promises aesthetic and functional rehabilitation. Endoscopic rhinosurgery plays an important central part in this context: It achieves extraction of foreign bodies, debridement, restoration of drainage and ventilation, and reconstruction of dura and bony walls along the shortest access avoiding unnecessary destruction for exposure.
Operative Technique
Foreign Bodies
The extraction of foreign bodies from the paranasal sinuses and the rhinobasis is the domain of endoscopic surgery. Implanted through accidents with circular saws or grinding machines in the workplace, by catapults or play guns in gaming situations, by criminal gun shot, by road traffic accidents, or by impalement from dentistry or leisure activities (Fig. 9.1a, b) , the foreign objects are of various materials and sizes, and their position may be superficial or deep in the forehead. There may be no related symptomatology and the entry wound may be hidden.
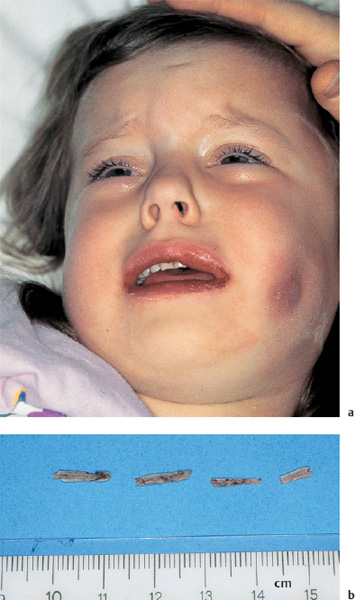
Fig. 9.1 a, b Impalement of the maxillary cavity.
a External aspect with swollen facial soft tissues but without visible fistula.
b Corn stalks after endoscopic removal (cm scale).
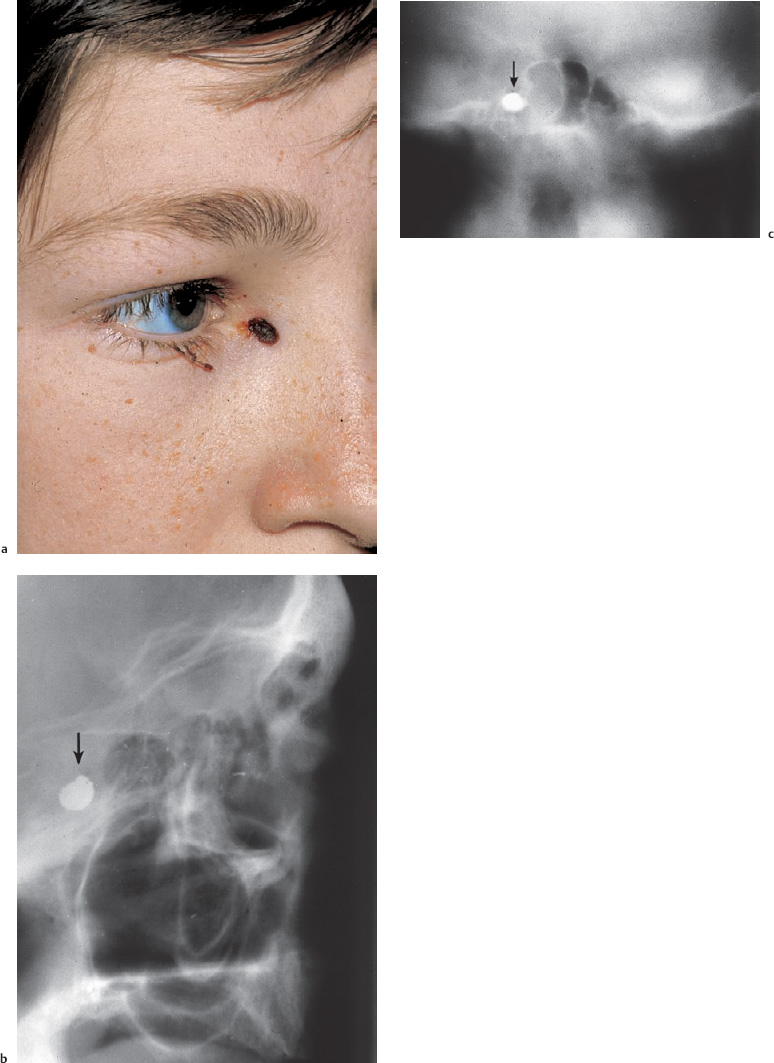
Fig. 9.2 a–c Intranasal endoscopic removal of a bullet impacted in the wall of the sphenoid sinus.
a Entry wound in the right medial canthus.
b Sagittal polytomography showing the position in the floor of the sphenoid sinus.
c The coronal section localizes the bullet lying in the lateral wall of the sphenoid sinus.
History taking in children is unreliable, hence pain or persistent suppuration may be the only hints of external pathogenesis. A thorough inspection and imaging by modern methods of ultrasound, CT, or MRI will localize the specimen (Fig. 9.2a–c) though these methods can fail with wood or plastic objects. One should always be aware that there may be several pieces.
The rhinosurgical exposure follows the techniques described in Chapter 6 on standard operations. Provided the subregion is healthy and not soiled, the endonasal access into the ethmoids and maxillary or sphenoid cavity will employ the shortest and most direct exposure Fig. 9.3). External surgery is usually not indicated. Mucosal reaction with hyperplasia and polyps, on the other hand, may require more extensive sinus surgery Fig. 9.4). An involved maxillofacial surgeon should be informed about the benefit of endoscopic equipment and the endonasal approaches lest unnecessary external operations are planned. Figure 9.2 gives an example of a transnasal sphenoidotomy for the removal of foreign bodies from the skull base. This projectile could be assessed by drilling the surrounding bone under microscopic control via a transnasal exposure of the sphenoid. Every defect in the skull base must be inspected and if necessary debrided. Packing and postoperative treatment are the same as for secondary healing after ethmoidectomy. Similar principles apply for the extraction of foreign bodies from the orbit.
Greater problems arise if multiple fragments have been forced into the frontal sinus or have penetrated the frontal skull base into the anterior cerebral fossa (Fig. 9.5a, b) . If they are limited to the sinus, a small oste oplastic sinusotomy is indicated. Revision of the anterior cerebral fossa is matter of a neurosurgical approach, but the anterior base of the skull is a relatively firm party wall between the paranasal sinuses and the frontal brain lobe that resists foreign bodies penetrating from below.
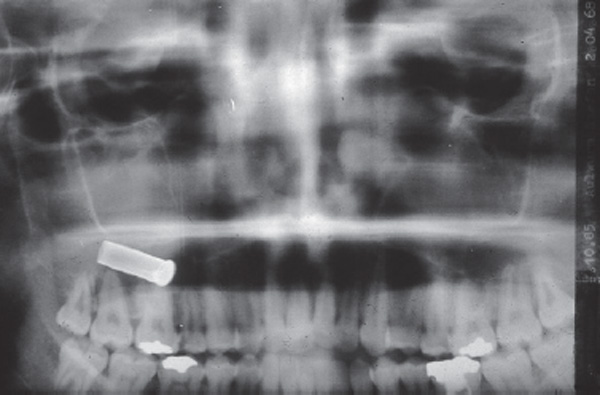

Fig. 9.4 Glass fragments in the left antrum initiating polyposis. The patient had presented with facial pain 3 years after the injury.
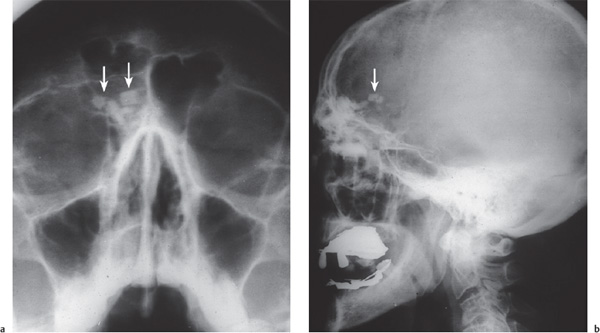
Fig. 9.5 a, b Intracerebral impalement of glass fragments from car accident.
a The frontal radiograph simulates foreign bodies in the frontal sinus (arrows).
b The lateral head projection makes obvious the endocranial, transbasal impalement (arrow), which was managed by a combined neurorhinosurgical approach.
If an asymptomatic foreign body is situated in close vicinity to a vital structure (internal carotid artery, optic nerve, etc.), its tissue-compatibility should be assessed, and the risks of an extraction must be weighed.
Open Injury
Sharp or blunt impalement and gun shot wounds, are not infrequently an origin of destruction within the infrabasal pneumatization of the skull base itself. If surgical management is indicated by inspection, imaging, or history, the intervention should aim at restoration of the natural infrastructure of bone and mucosa with their self-cleaning mechanisms. CT imaging is obligatory and will indicate whether osteoresynthesis with an external approach is necessary. All other measures such as internal debridement, refenestration, or removal of obstructive scar formation, and the management of late complications, can be achieved by endoscopy. The standard operations described above provide the guidelines. Wound closure is confined to external sutures of muscles, subcutis, and skin.
Midfacial and Orbital Fractures
Midfacial and orbital fractures, mostly accompanied by orbital hematoma (Fig. 9.6a, b) , can be regarded as closed injury and are managed as described in the preceding section. A majority of them will be referred to the maxillofacial services. Their surgical therapy does not always conform with rhinosurgical solutions, which offer the maximal preservation of the bony infrastructures together with restoration of disturbed ventilation and drainage of sinuses. Endoscopic standard operations thus provide a less invasive reconstruction of the maxillary or frontal sinuses (Smith et al. 2002) than the classic transoral and transfacial exposures still common in many centers.

Fig. 9.6 a, b Monocle hematoma from ethmoidal fracture.
a The typical facial aspect.
b Fractured bone fragments in the right ethmoid and from the medial and orbital wall impaling the orbit (coronal CT).
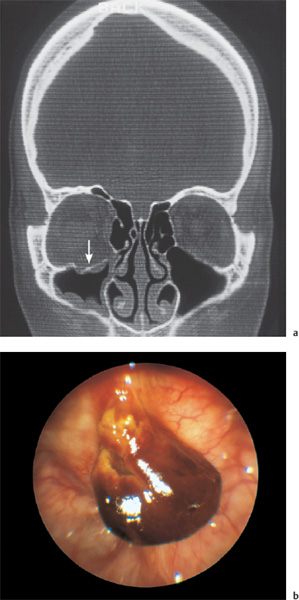
Fig. 9.7 a, b Blowout fracture of the right orbit.
a The fracture visible (arrow) in a coronal CT projection.
b The endoscopic view of the fracture with hematoma in the antral roof (70° telescope).
Blowout fractures and other injuries of the orbit, on the other hand, are only exceptionally suitable for purely endoscopic approaches (Fig. 9.7a,b) . They are more reliably treated by an infraorbital or transconjunctival access giving better opportunity for muscular repair and for the solid interposition of a new orbital floor, but can sometimes be mastered by an endoscopic transcanine approach (Strong et al. 2004). Lateral frontal sinus impression fractures require an external reconstruction.
Anterior Skull Base Fractures
The anterior part of the anterior skull base is formed by the posterior wall of the frontal sinus and the roof of the orbit. In the middle lies the roof of the ethmoid, and posteriorly the sphenoid plane and the roof of the sphenoid sinus see Fig. 6.80). The description in the previous section of the exposure of the ethmoid and sphenoid roof with the intranasal endoscopic technique related only to dissection of the anterior skull base from below. The posterior wall of the frontal sinus is suitable for only very limited endoscopic manipulations, especially if laterally fractured (Fig. 9.8a, b) , but the lateral and posterior walls of the sphenoid sinus are well within the reach of endoscopy.
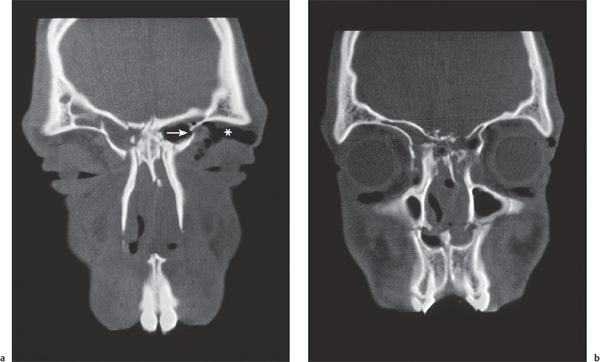
Fig. 9.8 a, b Lateral fracture of the left frontal sinus (arrow) with injury of the skull base requiring an external approach (coronal CT).
a Comminuted bilateral fracture of the anterior ethmoidal roof on the right side (arrow) and left frontal sinus impression causing subdermal emphysema (*).
b A more dorsal section shows crushed ethmoids, indicating endoscopic ethmoidectomy. Also destruction of both maxillae and of the nasal septum is visible.
Anterior ethmoidectomy is the method of choice for access to the base of the skull, followed by posterior ethmoidectomy with opening of the sphenoid sinus and exploration of the frontal sinus infundibulum. Individual circumstances will decide the extent of the exposure of the base of the skull. Particular procedures do not need to be described further at this point. Ethmoidectomy in these circumstances naturally includes the radical removal of the mucosa as far as this is necessary for the inspection of the underlying bone.
The inelastic periosteum of the anterior cranial fossa is tightly anchored on the bone, in contrast to the internal periosteal lining of the calvaria. This explains why skull base fractures regularly tear the overlying dura. Even if rhinoliquorrhea is not prominent, a suspicion of a hidden dural defect with danger of ascending meningeal infection must arise and calls for careful diagnosis. This consists of an endoscopic visualization of fl uorescence in the nasal cavity after suboccipital application of sodium fluorescein (1 mL of a 5% solution), using an ultraviolet light source.
A less aggressive test is the detection of β-II transferrin in nasal swabs after its administration. This amino acid is selectively accumulated in the cerebrospinal fluid. Such tests are in fact superfluous if CT or MRI has shown intracranial presence of air. Figure 9.9 shows an example of a large pneumatocele. More often, small trains of air bubbles cover the cerebral cortex and are thus easy to overlook.
The length of the fracture gap need not correspond to the width of the dural rupture. Its full endoscopic exposure appears prudent, however, in order to avoid overlooking other fistulas. Larger destructions with a diameter of more than 2–3 cm, especially comminuted fractures and bilateral disruption, are managed by a transfacial or an external trans cranial–or perhaps bitemporal–neurosurgical approach. This must be regarded as an emergency indication implemented in craniocerebral trauma immediately after stabilization of the patient’s vital functions. Another question is the optimal timing of the surgical treatment of concomitant midface fractures, either simultaneously or delayed. Individual strategies depend on good cooperation between neurosurgeon, rhinosurgeon, and maxillofacial surgeon. In recent years, neurosurgical interventions have always been given absolute priority Fig. 9.10). This was followed by two subsequent operations–in the same session or staged with delayed reconstruction of the midface bones, according to the individual dimension of bone displacement. Endoscopic revision of infractured ethmoids and other paranasal sinuses could often be postponed or even discarded because of spontaneous reventilation. A fresh CT scan may easily be misinterpreted and prompt unnecessary endoscopic resections because of opacity due to traumatogenous hemorrhage and acute mucosal swelling. Careful rhinological monitoring will eventually identify failures of the closure of dural defects and indicate endoscopic revision of remnant fistulas. The transition between posterior ethmoid and sphenoid is a particularly problematic zone. Persistent CSF leaks here can be closed with little effort under microscopic or endoscopic control using the endonasal technique described above. The posterior wall of the frontal sinus, however, is suitable only for very limited endoscopic manipulations.
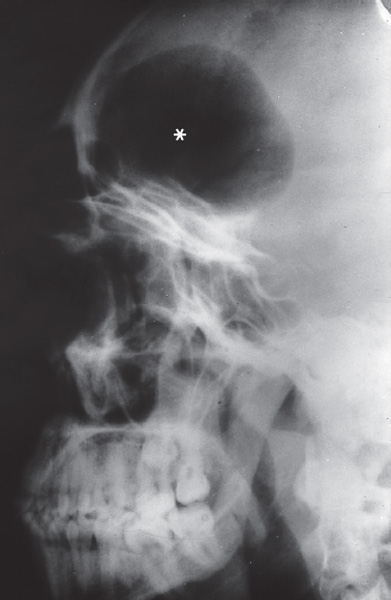
Fig. 9.9 Large pneumatocele (*) above the anterior skull base, indicating a dural fistula after car accident (sagittal radiograph).
For an ethmoidal–dural fistula, confirmed by CT, an approach via the middle meatus (preserving the middle turbinate), the ethmoid infundibulum, and the ethmoid bulla or via the common nasal meatus is suitable (Fig. 9.11a, b) . In the absence of polyposis, this dissection can be very precise. If a fracture line crossing the olfactory cleft causing a CSF leak is expected, surgery should begin with a partial resection of the middle turbinate so that the base of the skull can be inspected endoscopically in the midline along the medial lamella of the middle turbinate without obstruction by the body of the middle turbinate. If an iatrogenic CSF leak after a previous ethmoid operation requires closure, the surgery must be adapted to the prevailing situation, beginning with systematic removal of scar tissue and gradual exposure of the bony base of the skull by removal of any remaining cells.
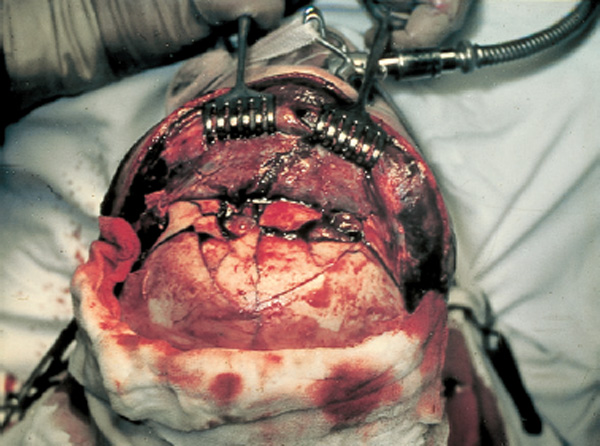
Fig. 9.10 Bi-frontoparietal exposure of a larger comminuted fracture of the midface and calvaria requiring a combined endoscopic transnasal and external approach.

Fig. 9.11 a, b Endoscopic management of a skull base fracture at the ethmoido-sphenoidal transition.
a The incorporated graft after 8 months visible (*) above the broad entrance to the right sphenoid sinus. At the left margin is the supratubal torus (70° telescope).
b The vital graft below the bone defect is evidenced in coronal CT section (arrow).
The immediate repair of a CSF fistula caused by injury of olfactory fibers in the anterior and middle ethmoid roof has already been described in Chapter 6 (see pp. 135–137). The technique has proved to be reliable and has therefore also been developed as the standard procedure for traumatic and idiopathic dural fistulas of other types and sites. The decision between a wide external rhinological procedure, a transfrontal neurosurgical exposure of the anterior skull base, or an intranasal endoscopic access for closure of a CSF fistula should today depend on generally accepted guidelines (Wigand 1990; Herrera and Caicedo 2000; Sethi 2000; Lee et al. 2004). Tradition, a surgeon’s previous training, and the instruments available often carry too much weight in the decision. The advantages of intranasal debridement of a localized fracture of the base of the skull and closure of a dural defect include preservation of bony support of the floor of the frontal sinus, avoidance of division of the supraorbital nerve, and prevention of the permanent anosmia characteristic of the neurosurgical procedure.
The technique is not difficult if the surgeon is familiar with bimanual endoscopy. After removal of as much of the middle turbinate as necessary, the ethmoid cells are cleared up to the base of the skull. Once the fistula has been found (see Fig. 6.82 a) , the neighboring mucosa is removed delicately from the edge over a distance of 2–4 mm using fine curved double forceps. If the fistula reaches the nasal septum, removal of the mucosa must encompass this area.
After careful demarcation of the defect, a graft is fitted carefully over the fistula and the surrounding bone edges and fixed with tissue glue. A mucosal flap taken from the free edge of the inferior turbinate has proved very useful (Wigand 1981, 1990). Its interposition and stabilization with nasal forceps and an elevator is not particularly difficult but demands prior hemostasis and very careful use of the suction. The site of the graft must be checked carefully by endoscopy.
The graft’s margins have to overlap the adjacent healthy bone by at least 1–2 mm, and are fixed to the bone with fibrin tissue adhesive. This mucoperiosteal patch works as a free graft. It should fit snugly into the exposed area, and must not be laid over neighboring mucosa (see Figs. 6.26, 6.27). Skull base defects larger than 5 mm in diameter may require more solid plugging. A free graft of fascia lata of an adequate size should then be pushed below the bone margins; this is secondarily covered by the mucosal patch with application of fibrin glue.
The edges are then covered with a further layer of tissue glue. Once this is dry, the nose is packed with material such as fibrin foam, which is removed at the earliest from 2 to 3 weeks later. Indeed, it can be left until it is rejected spontaneously. The nasal packing of petrolatum gauze introduced beneath this contact packing can be removed as early as 10 days after the operation. Since healing of the transplanted tissue to the bone requires several weeks, reoperation should not be immediately embarked upon for a slight CSF leak in the first postoperative weeks. In this event it might be necessary to adjust the nasal packing, place the patient with the head in the upright position, and drain off CSF by a lumbar drainage.
As was mentioned in chapter 6, a similar procedure is followed in the roof of the sphenoid sinus (Fig. 9.12, see also Fig. 6.81). Details were described on page 136.
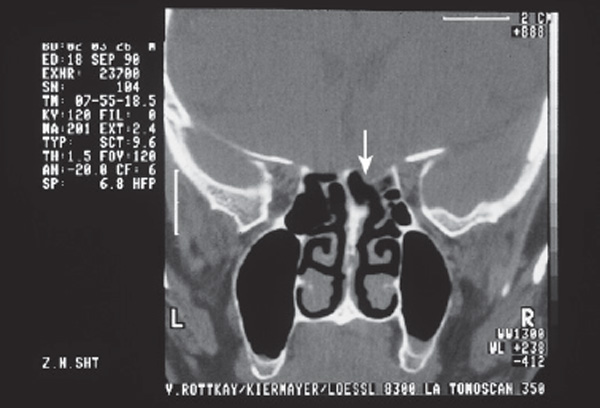
Fig. 9.12 Herniation of the injured dura (arrow) into the left ethmoid and sphenoid with skull base fracture (coronal CT).
An analysis of iatrogenic fistulas in a consecutive series of 24 patients, consisting of our patients and of preoperated patients from other services, that were treated at the department in Erlangen evidenced the following sites of dural injury :
| Anterior ethmoid, including nasofrontal duct | 12 |
| Frontal sinus infundibulum | 4 |
| Posterior ethmoid | 4 |
| Olfactory rim | 3 |
| Sphenoid cavity | 1 |
| and the kind of surgery for repair: | |
| Endonasal | 20 |
| Transfacial | 4 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


