Transoral Robotic Surgery (TORS) for Cancer of the Tonsil
Bert W. O’Malley Jr
INTRODUCTION
Many otolaryngologists believe that surgery for squamous cell cancer of the oropharynx is not routinely performed and that almost all patients are treated either with radiation alone or with chemoradiation. Over the past 30 years, radiation or chemoradiation has become the therapy most commonly recommended for the treatment of the majority of patients with cancer of the tonsil. The rationale for advocating nonsurgical therapy for advanced cancer of the tonsil was to avoid the significant morbidity associated with classic open approaches to the tonsil and the base of the tongue. These invasive open surgical techniques might include a lip-splitting incision, a mandibulotomy, major resections of noninvolved muscles and other soft tissues, tracheostomy, and the need for microvascular free flap reconstruction. However, in order to achieve similar oncologic outcomes for chemoradiation versus classic open surgery and postoperative adjuvant therapy, the radiation doses and volumes have been escalated in conjunction with multidrug chemotherapy regimens. Machtay et al. analyzed the late sequelae of all long-term survivors of chemoradiation in previously completed Radiation Therapy Oncology Group (RTOG) trials and found that 35 of 101 (34.6%) surviving patients with advanced oropharynx cancer had severe late toxicities (i.e., noncancer deaths attributable to treatment, fistula, tracheostomy, long-term feeding tube) following chemoradiation. In addition, a review of the literature in a recent publication about transoral robotic surgery (TORS) for oropharyngeal cancer identified a range of 8% to 38% chronic or long-term percutaneous gastrostomy (PEG) dependence in patients who received state-of-the-art intensity-modulated radiation therapy in combination with chemotherapy. These not-uncommon side effects raised the question as to whether less invasive surgical techniques would prove equally as effective oncologically with fewer functional sequelae than the current state-of-the-art chemoradiation regimens.
The surgical robot that is commercially available and used for current TORS procedures is the da Vinci robot (Intuitive Surgical, Sunnyvale, CA) (Fig. 13.1). The key benefits of the surgical robot include the high-magnification and three-dimensional optics that allows careful dissection, and identification of nerves and vessels, which facilitates en bloc resection. In addition, the instruments most commonly used are 5 mm in size and can be readily moved and manipulated within the oropharynx by the primary surgeon sitting at a remote console (Fig. 13.2). These small robotic instruments provide over 360 degrees of freedom of movement while allowing motion scaling and providing total tremor filtration, which adds significant precision to the surgical procedures. In addition to the primary surgeon operating from the console, there is ample room for a bedside assistant surgeon to also provide transoral suctioning and retraction with instruments in both hands. Thus, in principle, TORS is similar to the classic two-surgeon, four-handed surgery, except that it is performed using the robot. Specific steps and concepts that allow for safe and complete resection of cancer of the tonsil are outlined below.
Published studies from human trials have demonstrated both the feasibility and safety of TORS for cancer of the upper aerodigestive tract. These TORS procedures are associated with limited surgical morbidity, reduced hospitalization, and enhanced patient functional outcomes, particularly in swallowing, over present chemoradiation therapies. The long-term PEG dependency rates after TORS, in a series of patients
with advanced oropharyngeal cancer treated with TORS followed by neck dissection and adjuvant therapy as indicated, at the University of Pennsylvania have ranged from 2.4% versus 8% to 38% for chemoradiation for similar patient cohorts.
with advanced oropharyngeal cancer treated with TORS followed by neck dissection and adjuvant therapy as indicated, at the University of Pennsylvania have ranged from 2.4% versus 8% to 38% for chemoradiation for similar patient cohorts.
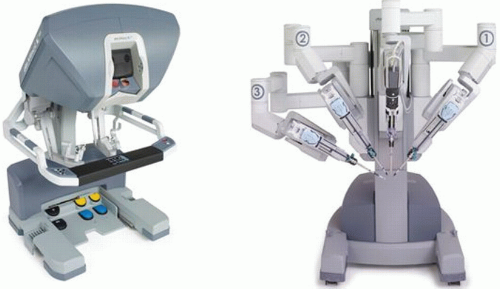 FIGURE 13.1 Photo of robot. |
Another factor to consider is the growing number of patients with cancer of the tonsil who have human papillomavirus (HPV) as an etiologic factor. These patients who are HPV positive have significantly improved cure rates when compared to patients who are HPV negative using radiation or chemoradiation strategies. Furthermore, the primary cancers are characterized by lower T stage in general, which are amendable to transoral resection. In our recent cohort study on the benefit and outcomes of TORS based on HPV status, we achieved equally successful high rates of survival and tumor control regardless of whether a patient is HPV positive or negative. For patients who are HPV positive, it may be a reasonable consideration to investigate “de-escalation” of therapy, and TORS for cancer of the tonsil may find a role in this concept.
HISTORY
The classic history for patients with squamous cell cancer of the tonsil from previous decades was that of a heavy smoker or smoker and drinker, typically a pack per day or more over 10 years with varying degrees of alcohol intake reported. In our present decade, the history has shifted to include an ever-increasing number of patients who report no smoking, or smoking in the distant past, and have a minimal history of alcohol intake. As mentioned above, these patients have a cancer, which is HPV positive, and thus the cause of their cancer is attributed to this viral infection, which occurred an estimated 20 to 40 years prior to the cancer.
This widespread prevalence is a key reason why oropharyngeal cancer is one of the most rapidly increasing cancers in the United States.
This widespread prevalence is a key reason why oropharyngeal cancer is one of the most rapidly increasing cancers in the United States.
 FIGURE 13.2 Photo of the 5-mm instruments. |
It is important to take a thorough past history on patients with an emphasis on the smoking and alcohol consumption. If the patient has significant medical comorbidities, then medical or cardiac clearance is always warranted. It is also important to perform HPV testing or its surrogate p16 expression by immunohistochemistry on fine needle aspirations of metastatic lymph nodes or biopsies of the primary cancer of the tonsil. The knowledge of HPV involvement may help drive the options of therapy, such as the consideration of de-escalated or minimally invasive combination therapies.
PHYSICAL EXAMINATION
A thorough examination of the head and neck is warranted, with particular attention to the size and extent of the primary cancer of the tonsil using transoral direct visualization and indirect laryngoscopy. Extension of the cancer of the tonsil into the nasopharynx or to the midline of the posterior pharyngeal wall is considered contraindication to TORS. While it is technically feasible to completely resect these more extensive cancers, I believe that the magnitude of removal of the constrictor muscle puts the patient at greater risk of near-term postoperative as well as persistent dysphagia, which is a complication of chemoradiation that TORS was intended to reduce.
The neck is palpated to identify lymph node metastases and allow basic clinical determination of fixation, which suggests the presence of extracapsular spread of the metastatic cancer. Another key clinical finding to evaluate is the presence of trismus, which is indicative of extension beyond the constrictor muscles into the pterygoid muscle. Extensive involvement of the pterygoid muscle is a contraindication to TORS, although minimal invasion of the medial pterygoid muscle is acceptable for TORS approaches.
INDICATIONS
Indications for TORS at the University of Pennsylvania have been based on the desire to ensure (1) a high percentage of cancer-free surgical margins; (2) excellent, reproducible, functional outcomes; (3) healing by secondary intention or if there is a soft palate defect, bone exposure, or carotid exposure, then use local flaps rather than free flaps; and (4) safety from the perspective of the major vasculature. I suggest that the reader keep these concepts in mind when reviewing our suggested indications and contraindications for TORS radical tonsillectomy.
The indications for TORS for cancer of the tonsil start with the ability of a patient to undergo surgery in general. In general, all T1, T2, T3, and selected T4 cancers as defined by the American Joint Committee on Cancer (AJCC) are amenable to TORS.
CONTRAINDICATIONS
In general, I consider patients with Stage IVc as not being candidates for surgery except if they have a solitary or curable pulmonary or other distant metastasis. In addition, the following are considered contraindications for TORS:
Cancers that are T4a except for cases where there is limited unilateral involvement of the ipsilateral base of the tongue or medial pterygoid muscle. This is assessed on physical examination, typically under general anesthesia, and is not a radiologic diagnosis.
Although deep extension across the midline of the base of the tongue is a contraindication for TORS based on the contention that bilateral resection of the base of the tongue could devascularize, the tongue and that loss of much greater than half the deep tongue base may be functionally debilitating. Of note, superficial extension of cancer (i.e., mucosal involvement without deep muscle invasion) to the contralateral tongue base is not a contraindication to TORS.
AJCC T4b tumors indicate cancer extension into the lateral pterygoid, or encasement of the carotid artery, or significant bone invasion. For patient safety considerations in the TORS approaches, I feel that any cancer, which abuts the internal carotid artery or carotid bifurcation, should be considered a contraindication. While some authors have advocated the use of free flap reconstruction following wider resections with TORS, it is our contention that since squamous cell carcinoma that abuts the carotid system may be adherent, dissection of the carotid transorally should be avoided.
Involvement of the pharynx at, or across, the midline, extension into the nasopharynx, or invasion of the prevertebral fascia are contraindications. It is important to note that while this lateral or deep invasion may be identified on computed tomography (CT) or magnetic resonance imaging (MRI), nevertheless palpation of the cancer under anesthesia is critical to confirm these findings.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


