Transoral Excision of Cancer of the Tonsil
Roberto A. Lima
INTRODUCTION
Cancer of the oropharynx represents 10% to 15% of all cancers of the head and neck. Most of these cancers (50%) occur in the tonsil region, including the tonsil, tonsil fossa, and tonsil pillars.
Unfortunately, most of these cancers are identified in advanced stages. The indolent progression, as well as large number of lymphatics, and a common confusion with infection have been suggested as to why these cancers are diagnosed in advanced stages.
The use of radiotherapy alone or chemoradiation has been the primary treatment option in many centers around the world. Recently the association of cancer of the oropharynx with human papillomavirus has been described and explains the increased incidence of this tumor in young patients.
The tonsil fossa, which contains the tonsil, is limited by the anterior tonsillar pillar (palatoglossus muscle) and the posterior tonsil pillar (palatopharyngeal muscle).
Lateral to the tonsil fossa are the pharyngeal muscles, the mandible, and the parapharyngeal space. The carotid artery is just lateral and posterior to the tonsil fossa. In this region, special care should be taken to avoid injury to these structures (Fig. 12.1).
HISTORY
Most cancers of the oropharynx are diagnosed in advanced stages. Unfortunately, symptoms produced by the cancer are similar to the infections commonly occurring in this area. A vague, suggestive discomfort, scratchy feelings, and minor otalgia are often treated with antibiotics without a diagnosis for some months. The occurrence of a cervical mass is the primary symptom in 25% of the patients.
The occurrence of pain in the throat, mainly while swallowing, is a very common symptom along with the occurrence of otalgia which is caused by invasion of the glossopharyngeal nerve. The pain reaches the ear by connections with the petrosal ganglion and Jacobson (tympanic) nerve. The occurrence of bleeding and trismus is more common in cases of advanced cancer. Voice changes can be present in cases of invasion of the base of the tongue.
PHYSICAL EXAMINATION
A careful clinical examination must be done with inspection and palpation including the parapharyngeal space for correct staging of the primary cancer of the oropharynx and the neck. Infiltration of the oral tongue, the base of the tongue, and the vallecula is identified by palpation. Many times this infiltration is submucosal, preventing direct visualization. This examination is very important before the surgery because invasion of these structures is a contraindication to surgery.
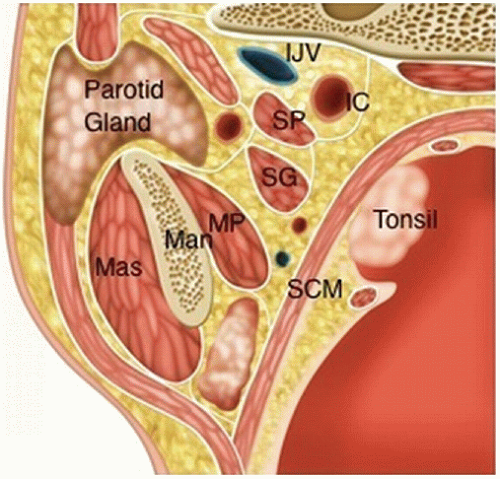 FIGURE 12.1 Anatomic structures located in the tonsil region. IC, internal carotid artery; IJV, internal jugular vein; Man, mandible; Mas, masseter muscle; MP, medial pterygoid muscle; parotid gland; SG, styloglossus muscle; SP, stylopharyngeus muscle; SCM, superior constrictor muscle; and tonsil. |
INDICATIONS
Squamous cell carcinoma of the tonsil can be adequately resected through the oral cavity. However, some characteristics should be respected. The stage of the cancer (T1/T2) is most important; we understand that advanced cancer is a formal contraindication because of the relationship between this region and the carotid artery and mandible laterally.
Some authors have reported their experience with resection of more advanced cancer of the tonsil fossa, even for T3 lesions. One study included a series of 166 cases using an incision in the mucosa of the anterior pillar reaching a dissection plane between the buccinator and the superior constrictor muscle using the superior constrictor muscle as the deep margin (Fig. 12.2).
In some cases, metastasis to the cervical lymph nodes may be the first symptom of a very small cancer of the tonsil. In these cases, the tonsil can be resected through the oral cavity and a neck dissection performed at the same sitting.
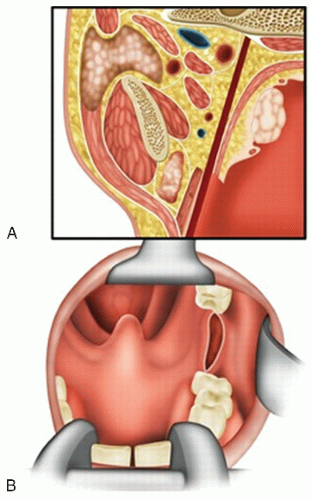 FIGURE 12.2 A: The dark line demonstrates the dissection plane to reach a safe margin and protect the internal carotid artery. B: The incision should be done on the pterygomandibular raphe, where the buccinator muscle and superior constrictor are fused. |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


