Transoral Endoscopic Laser Treatment of Early Glottic Cancer
Steven M. Zeitels
INTRODUCTION
Transoral endoscopic removal of glottic cancer was reported first in 1888 as a mirror-guided piecemeal resection approach. Approximately 30 years later, Lynch reported a bimanual, direct, suspension laryngoscopic method, which was later enhanced by the magnification provided by the surgical microscope. In the early 1970s, Jako, Strong, and Vaughan introduced a carbon dioxide laser that was coupled to the surgical microscope, which ultimately became the watershed innovation that facilitated widespread adoption of endolaryngeal cancer surgery. In recent years, fiber-based delivery systems have further enhanced this method by providing substantially better control of the operative field.
Given the long successful history of endoscopic treatment of early glottic cancer, there is no controversy about its feasibility and success. Unlike other sites of the upper aerodigestive tract, early glottic cancers (T1/T2) rarely metastasize, which provides unique opportunities for staged treatment strategies. Furthermore, since the cure rate is extremely high for any surgical approach or radiotherapy, the key metric for success in our communication-based society is predicated on the voice outcome. It is also important to preserve future treatment options.
Optimal voice preservation is improved by the surgeons’ keen awareness of vocal physiology. This understanding of the functional aspects provides insights into the impact on the voice of a spectrum of neoplastic lesions prior to treatment, subsequent to resection, and after phonosurgical reconstruction. The reconstructive strategies are designed to enhance aerodynamic glottal competency. For most patients treated for early glottic cancer, the primary sound source is the uninvolved phonatory mucosa of the vocal fold. Results are improved if this mucosa is spared exposure to radiation treatment or other intervention, which generates fibrosis and scar.
Noncancer phonatory mucosa is driven into oscillation by preserving or reestablishing aerodynamic competency after the tumor is treated. This is achieved by (1) minimizing soft tissue removal through extremely narrow margins; (2) preserving the architecture of the rima glottidis by means of metachronous treatment of each vocal fold, thereby preserving the structure of the anterior commissure; and (3) reconstructing the paraglottic compartment by means of transoral and/or transcervical medialization procedures if an extensive amount of vocal musculature has been removed.
Approximately 7 years ago, I abandoned CO2 laser excision of early glottic cancer in favor of angiolytic laser involution of the disease so that we could maximize preservation of glottal soft tissue. This has been done primarily with the use of the 532-nm GreenLight KTP laser. More than 75 patients have been treated by this technique with control rates of approximately 95% for T1 cancers and 75% for T2 cancers. Furthermore, the majority of patients with T2 cancers are salvaged with radiotherapy, thereby saving this valuable single-use treatment option in most patients. Moreover, KTP laser treatment resulted in our best voice results to date while not compromising cure of the cancer when using ultra-narrow margins.
HISTORY (Video 22.1)
The primary and key symptom for patients presenting with early glottic cancer is that of vocal dysfunction and hoarseness. Apart from a harsh coarse vocal timber, patients may describe difficulties with pitch variation, pitch breaks, and vocal fatigue and difficulties with projection in settings where there is substantial ambient noise. Most commonly, friends, colleagues, and especially new contacts inquire if he/she is “sick.” Airway difficulties, hemoptysis, otalgia, and dysphagia are rare symptoms with early glottic cancer.
PHYSICAL EXAMINATION
Distal-chip flexible laryngoscopy should be done with extremely close proximity to the tumor to define the perimeter of the lesion. To the extent that it is possible in the outpatient setting, the tumor edge should be defined laterally in the ventricle, caudally with relation to the inferior arcuate line and the superior area of the subglottis, anteriorly at the anterior commissure, and posteriorly around the arytenoid cartilage. These findings should be recorded by photos or video. This examination can be enhanced by narrowband imaging, which often highlights angiogenic dysplasia at the perimeter of the lesion.
Stroboscopic examination of the phonatory mucosa can be done with a rigid telescope (Video 22.2; Fig. 22.1A and B) or a flexible laryngoscope. Stroboscopy is valuable in selected circumstances for determining the depth of a neoplasm if a patient has not had extensive biopsies, undergone prior treatment of dysplasia, or had sustained long-term phonotrauma. More importantly, stroboscopic assessment of the glottis provides an assessment of residual pliable superficial lamina propria (SLP), which will be the oscillatory sound source for the patient once the tumor has been successfully treated and aerodynamic competency of the glottal valve reestablished.
Vocal cord mobility must be determined in order to adequately stage the patient’s cancer. Diminished mobility may occur from mass involvement of the intrinsic muscles of the paraglottic space or by direct involvement of the cricoarytenoid joint. A T2 cancer may be designated as such due to either surface involvement of either the supraglottis or subglottis or if there is impaired mobility of the glottis. In my opinion, there is greater success in treating T2 cancers with surface involvement of two mucosal subsites compared to impaired mobility due to deep tumor invasion.
INDICATIONS
The indications for endoscopic resection of early glottic cancer include T1a and T1b cancers as well as selected T2a and T2b cancers. It is possible to treat these cancers after failed radiotherapy, but the oncologic and functional results are not as good as with primary treatment. The decision to proceed in cases of radiation failure should be individualized based on the original size and location of the cancer, endoscopic exposure, imaging studies, expectations and motivation of the patient, equipment available, and skill sets of the surgeon.
CONTRAINDICATIONS
The most common contraindication to effectively removing a glottic cancer endoscopically is the inability to fully visualize the neoplasm during suspension laryngoscopy. This primarily occurs due to restrictions in visualization of the anterior glottis due to the anatomy of the patients’ oral cavity, mandible, and neck. Some examples of these
problems include limited mouth opening, a narrow mandibular arch or torus deformities, and/or limited or narrow oropharyngeal inlet with relative macroglossia. It may also occur due to limitations of extension at the atlantooccipital joint or severe fibrosis of the soft tissues of the neck secondary to radiation or burns. Less commonly, a neoplasm has an unfavorable pattern of invasion so that despite reasonable laryngoscopic exposure, it cannot be reliably eradicated. Typically, these problems are determined during the preoperative evaluation.
problems include limited mouth opening, a narrow mandibular arch or torus deformities, and/or limited or narrow oropharyngeal inlet with relative macroglossia. It may also occur due to limitations of extension at the atlantooccipital joint or severe fibrosis of the soft tissues of the neck secondary to radiation or burns. Less commonly, a neoplasm has an unfavorable pattern of invasion so that despite reasonable laryngoscopic exposure, it cannot be reliably eradicated. Typically, these problems are determined during the preoperative evaluation.
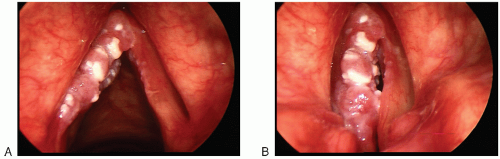 FIGURE 22.1 A: T2b carcinoma of the left vocal fold seen during abduction. The lesion crosses the anterior commissure to the contralateral right vocal fold. It extends past the inferior arcuate line caudally to the upper subglottis. The superior-lateral extent of the disease on the ventricular surface of the vocal fold cannot be determined on this examination. There is normal vocal fold mobility. B: On adduction and stroboscopy, there is no mucosal wave seen in the left vocal fold, and it is impaired on the right. |
Severe cardiopulmonary disease precluding general anesthesia is rare but certainly occurs. Anticoagulation is a relative contraindication based upon the size of the tumor, the difficulty in exposure, and the laser technology that is available. Fiber-based lasers are easier to use in patients who are anticoagulated. This is especially true for the KTP laser and the thulium laser. Understandably, cancer that invades cartilage or escapes through the connective tissue of the laryngeal framework is not generally considered to be suitable for an endoscopic procedure.
PREOPERATIVE PLANNING
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


