Transoral and transcervical surgery to treat glottic cancer has advanced substantially over the past decade. There have been considerable innovations that enhance vocal function for early disease and airway function for advanced disease. The fiber-based angiolytic 532 nm potassium titanyl phosphate laser has provided a new foundational strategy to maintain high cure rates with enhanced vocal outcomes for the treatment of early glottic disease. For advanced glottic cancer, transplanting cryopreserved aortic homograft to reconstruct wide-field laryngotracheal airway defects can provide an adequate airway caliber such that a long-term tracheotomy can frequently be avoided.
Key points
- •
Fiber-based 532 nm potassium titanyl phosphate (KTP) laser treatment of early glottic cancer combines the selectivity and precision of microsurgery with discreet zonal nonionizing radiation (photoangiolysis) integrating the assets of both conventional surgery and radiotherapy.
- •
Early glottic cancer can be optimally managed oncologically and with regards to voice outcome by means of photoangiolysis using the 532 nm KTP laser.
- •
Early glottic cancer that invades both vocal cords can be removed in 2 (staged) procedures so as to preserve the anatomic architecture of the anterior commissure and thereby achieve a better voice result as compared to a single procedure.
- •
Radiotherapy can be preserved as an oncologic treatment option in over 90% of patients with early glottic cancer, so that this single-use cancer treatment can be preserved for metachronous larger lesions.
- •
Transplantation of cryopreserved aortic homograft can be used effectively to restore the airway caliber in wide-field partial laryngectomy defects for advanced glottic cancer that extends subglottically.
Early glottic cancer
Background
Transoral endoscopic removal of glottic cancer was reported first in 1888 as a mirror-guided piecemeal resection approach. Approximately 30 years later, Lynch reported a bimanual, direct, suspension laryngoscopic method that was later enhanced by the magnification provided by the surgical microscope. In the late 1960s and early 1970s, Jako, Strong, and Vaughan introduced a carbon dioxide laser that was coupled to the surgical microscope, which ultimately became the watershed innovation that facilitated widespread adoption of endolaryngeal cancer surgery. In recent years, fiber-based delivery systems have further enhanced this method by providing substantially better control of the operative field.
Given the long successful history of endoscopic treatment of early glottic cancer, there is no controversy about its feasibility and success. Unlike other sites of the upper aerodigestive tract, early glottic cancers (T1 and T2 tumors) rarely metastasize, which provides unique opportunities for staged treatment strategies. Furthermore, because the cure rate is extremely high for any surgical approach or radiotherapy, the key metric for success in today’s communication-based society is predicated on the voice outcome. It is also important to preserve future treatment options.
Optimal voice preservation is improved by the surgeon’s keen awareness of vocal physiology. This functional understanding provides insights into the voice impact of a spectrum of neoplastic lesions prior to treatment, subsequent to resection, and after phonosurgical reconstruction. The reconstructive strategies are designed to enhance aerodynamic glottal competency. In the overwhelming majority of patients treated for early glottic cancer, the primary sound source is the remaining phonatory mucosa that is not involved with the cancer. It is also valuable to maintain adequate mucous hydration, which is provided by the glands of the saccule. Therefore, avoiding ionizing radiation to normal-residual phonatory mucosa and the saccular glands is advantageous.
Noncancerous phonatory mucosa is driven into oscillation by preserving or re-establishing aerodynamic competency after the tumor is treated. This is achieved by
Minimizing soft tissue removal through extremely narrow margins
Preserving the architecture of the rima glottidis by means of metachronous treatment of each vocal fold and preserving the structure of the anterior commissure
Reconstructing the paraglottic compartment by means of transoral and/or transcervical medialization procedures if an extensive amount of vocal musculature has been removed
Endoscopic Angiolytic Potassium Titanyl Phosphate Laser Treatment of Early Glottic Cancer
Approximately 8 years ago, the author abandoned carbon dioxide laser excision of early glottic cancer in favor of angiolytic laser involution of the disease in order to maximize preservation of glottal soft tissue. Angiolytic laser removal of early glottic cancer with ultranarrow margins was first published in a pilot study 6 years ago as an innovative surgical treatment strategy to better preserve vocal function.
It is likely that this was the first demonstration of employing nonionizing radiation without chemical enhancement (eg, photosensitizing agents) to involute and treat cancer without resection or gross ablation. This approach combines elements of surgery and radiation to create a unique hybrid approach.
Considering that the 3 conventional cancer treatments (surgery, radiotherapy, cytotoxic chemotherapy) evolved from the primary basic sciences (biology, physics, chemistry) Folkman’s conception of antiangiogenesis agents became the fourth cancer treatment. However, these agents are used as an adjuvant with other conventional treatment modalities. Based on discussions with Dr J. Folkman (personal communication, 2007), photoangiolytic laser treatment of the glottis is likely the first single-modality organ cancer treatment, which capitalizes on his philosophy that tumors retain denser blood supply and microcirculation as compared with normal surrounding soft tissue.
Photoangiolytic treatment of aerodigestive tract cancer has been done primarily with the 532 nm green-light KTP laser. The author had introduced angiolytic lasers (585 nm pulsed-dye laser, 532 nm pulsed-KTP laser) to facilitate microflap resection of glottal dysplasia in the late 1990s. Then, photoangiolysis of the subepithelial microcirculation allowed for extremely precise microflap epithelial resection, preservation of histopathological architecture, and minimal collateral thermal damage to the perivascular superficial lamina propria (SLP).
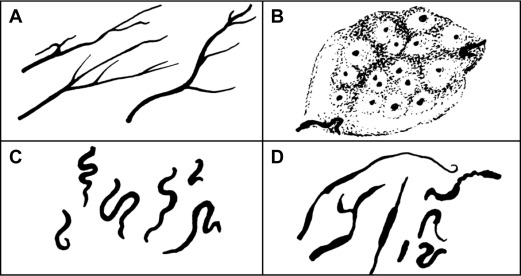
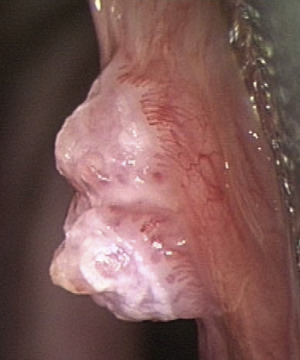
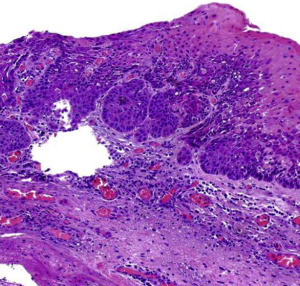
The promise of the angiolytic laser treatment of early glottic cancer was supported by concepts of aberrant neovascularity described by Jako and Kleinsasser ( Fig. 1 ) in 1966 and intralesional tumor angiogenesis ( Figs. 2 and 3 ) established by Folkman shortly thereafter in 1971.
During the past 8 years, over 200 glottic cancers have been treated by 532 nm KTP photoangiolysis, and results of a cohort with long-term follow-up were recently published. In that investigation, 117 patients (T1a-71, T1b-11, T2-10 unilateral/25 bilateral) underwent KTP laser treatment of early glottic cancer with a minimum 3-year follow-up (average: 53 months). Disease control for T1 and T2 lesions was 96% (79/82) and 80% (28/35), respectively. All 10 recurrences were treated with radiotherapy. Fifty percent (5/10) were controlled with radiotherapy, and the other 5 patients died of disease. Larynx preservation and survival were achieved in 99% (81/82) of patients with T1 disease and 89% (31/35) of patients with T2 disease.
This investigation provided clear evidence that angiolytic KTP laser treatment of early glottic cancer with ultranarrow margins was an effective surgical treatment strategy. Radiotherapy was preserved as an oncologic option for future use in 94% of patients and effectively salvaged half of patients who failed endoscopic treatment.
The voice results that the author achieved with angiolytic KTP laser treatment were superior to what could be achieved in the past with the CO 2 laser. This is especially so for those patients who have bilateral disease. Pretreatment and post-treatment voice outcome data were obtained for 92 patients (T1-64, T2-28) who underwent 532 nm KTP-laser treatment of early glottic cancer utilizing a design in which each patient essentially served as his or her own control. Evaluations included objective measures (acoustic and aerodynamic) and patients’ self-assessments of vocal function (voice-related quality of life, VRQOL). A series of mixed Analysis of variance with tumor stage and depth of invasion as the between-subject variables and time (before surgery vs after surgery) as the within variables was conducted for all vocal function measures.
There are several reasons for the improved voices, all of which can be explained by improvements in post-treatment aerodynamic competency of the glottis and/or enhanced phonatory mucosal pliability. Both were achieved through increased preservation of glottal soft tissue including noncancerous superficial lamina propria, the layer necessary for glottal vibration and optimal architecture of the rima glottidis.
Unlike prior microlaryngeal laser techniques that are used exclusively as a scalpel or indiscriminate ablating device (eg, CO 2 , continuous-wave KTP, Thulium, Pleasanton CA), angiolytic lasers concentrate the energy within the dense aberrant angiogenic microcirculation of the tumors while not penetrating deeply into the normal soft tissue of the vocal fold. Thick tumors are vaporized in a continuous wave mode with simultaneous cooling until the interface with normal underlying soft tissue. The interface is treated in a pulsed mode, and frozen section margins are obtained from the patient to establish that the tumor has been removed.
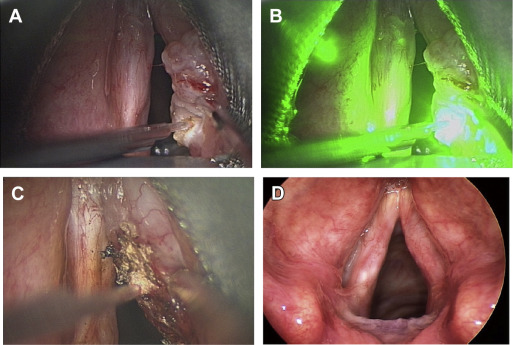
By confining the pulse-width to no more than 15 milliseconds, the angiolytic laser induces selective heating of the lesions’ intralesional/subepithelial microcirculation. This minimizes thermal trauma and fibrosis of the extralesional underlying normal glottal soft-tissue, thereby optimally preserving vocal fold soft tissue necessary for phonatory vibration. Photoangiolytic pulsed-laser treatment of early glottic cancer has the capability of preserving paraglottic space soft tissue in deeper neoplasms as well as mucosal SLP in more superficial tumors ( Fig. 4 ).
Cancer involvement of the anterior commissure tendon and/or the arytenoid cartilage is not a contraindication to this technique if adequate laryngoscopic exposure can be obtained. Thyroid cartilage invasion is a contraindication to this approach and requires transcervical removal of the thyroid lamina. To preserve the architecture of the anterior commissure, it is common to remove tumors with bilateral disease in 2 stages.
Two-staged pulsed photoangiolytic laser treatment by surgeons using nonionizing radiation retains elements of current phonomicrosurgery and radiotherapy models synthesizing key assets of both and comprises a significant revision of the typical surgical paradigm, which implies effective management as a solitary intervention. This is in contradistinction to radiotherapy and chemotherapy, which are incremental. For the promise of enhanced function, these nonsurgical cancer treatments have achieved acceptability despite the fact that patients have intercurrent disease during months of treatment. Moreover, it has been commonplace for decades for patients with advanced primary disease and regional metastasis to undergo incremental chemotherapy and radiotherapy (XRT) while intercurrent disease is left for 3 to 6 months. Considering this, and the fact that from microlaryngoscopic biopsy to completion of XRT is typically at least 2 months for early glottic cancer, there is no reason to believe that incremental staged endoscopic surgical treatment over the same time period will result in added risk to patients.
Salvage Endoscopic Angiolytic Potassium Titanyl Phosphate Laser Treatment of Early Glottic Cancer
Management of early glottic cancer subsequent to failed radiotherapy is challenging, especially balancing oncologic control and function preservation. Patients have frequently been incentivized against surgical management, which is why radiotherapy was selected as initial treatment. This orientation compounds the difficulty in discussions about surgical management after recurrence. Typically, endoscopic salvage is less morbid than transcervical partial laryngectomy and clearly desirable over total laryngectomy. However, there are appropriate concerns about the efficacy of endoscopic salvage and the overarching impact on larynx preservation and survival.
Given the success with endoscopic angiolytic KTP laser treatment of previously nonradiated T1 and T2 glottic cancer, the author examined previous results treating similar-sized lesions after failed radiotherapy. This investigation reported on the first 20 patients who failed radiation therapy elsewhere for early glottic cancer and were treated by endoscopic angiolytic KTP laser treatment.
The presentation of the geographic tumor recurrence in the 20 patients revealed T1aN0M0-4, T1bN0M0-1, T2aN0M0–1, and T2bN0M0–14. After KTP laser salvage treatment, 4 of 20 patients (20%) developed local recurrence (all bilateral T2) and required subsequent total laryngectomy; 3 of 20 patients (15%) ultimately died of disease. The remaining 16 patients (80%) were free of disease at least 2 years subsequent to endoscopic salvage, with an average follow-up of 39 months.
This investigation provided preliminary evidence that angiolytic KTP laser salvage treatment of early glottic cancer is an effective treatment after failed radiation. Larger cohorts and longer follow-up are necessary to establish incontrovertible efficacy.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


