The goal of this review is to facilitate an improved understanding of the indications and contraindications to transcervical conservation laryngeal surgery in the treatment of glottic and supraglottic carcinoma. An overview of seminal anatomic principles is presented to provide guidance for clinicians contemplating open partial laryngectomy options.
Key points
- •
In order to appropriately manage and counsel patients with laryngeal cancer, the physician must not only be aware of the armamentarium of treatment options, but also have a thorough understanding of the complex laryngeal anatomy that impacts tumor growth and behavior.
- •
Surgical and nonsurgical approaches should be considered with appropriate referrals as indicated; surgical options include transoral and transcervical approaches.
- •
The fibroelastic framework of the larynx provides distinctive barriers that may limit tumor extension in the early stages, but also guide predictable migration patterns in advanced cases.
- •
The paraglottic spaces form a conduit for extension to different laryngeal regions, which must be understood to better determine optimal treatment options.
- •
Understanding the distinctive anatomic associations within the larynx will enhance tumor mapping, and allow for superior outcomes.
Background
The understanding of the complex 3-dimensional anatomy of the larynx presents as a challenge to many beginning surgeons and clinicians. When presented with carcinoma of the larynx, an insufficient grasp of this intricate landscape may hamper the clinician’s ability to adequately counsel, refer, and direct appropriate therapeutic options for the patient. The objective of this article is to enhance the reader’s understanding of the critical anatomic structures that influence the evolution of laryngeal carcinoma and its functional impact on the larynx, in order to define the indications and contraindications of conservation laryngeal surgery.
Conservation options in ablative laryngeal surgery include both transoral and open transcervical approaches. The mainstay surgical treatment option for most early lesions is typically via a transoral approach, with shorter hospitalizations, lower morbidity, and improved functional results. However, this review will focus on transcervical approaches and discuss their seminal anatomic principles. Open approaches can be considered in situations where exposure is inadequate for transoral resection, or the transoral technique is not in the purview of the institution, as well as for salvage surgery after radiation failure. This topic will serve as a guide for clinicians seeking to understand management options beyond transoral laser surgery, radiation therapy, and total laryngectomy.
The different categories of open organ preservation surgery and their indications and contraindications will be summarized. The anatomic bases for these indications will be subsequently described.
Background
The understanding of the complex 3-dimensional anatomy of the larynx presents as a challenge to many beginning surgeons and clinicians. When presented with carcinoma of the larynx, an insufficient grasp of this intricate landscape may hamper the clinician’s ability to adequately counsel, refer, and direct appropriate therapeutic options for the patient. The objective of this article is to enhance the reader’s understanding of the critical anatomic structures that influence the evolution of laryngeal carcinoma and its functional impact on the larynx, in order to define the indications and contraindications of conservation laryngeal surgery.
Conservation options in ablative laryngeal surgery include both transoral and open transcervical approaches. The mainstay surgical treatment option for most early lesions is typically via a transoral approach, with shorter hospitalizations, lower morbidity, and improved functional results. However, this review will focus on transcervical approaches and discuss their seminal anatomic principles. Open approaches can be considered in situations where exposure is inadequate for transoral resection, or the transoral technique is not in the purview of the institution, as well as for salvage surgery after radiation failure. This topic will serve as a guide for clinicians seeking to understand management options beyond transoral laser surgery, radiation therapy, and total laryngectomy.
The different categories of open organ preservation surgery and their indications and contraindications will be summarized. The anatomic bases for these indications will be subsequently described.
Guiding principles and understanding of tumor spread
One should have familiarity with the complex normal laryngeal anatomy and the ability to establish an accurate assessment of tumor extent. Tumor mapping is performed through a combination of office-based, surgical clinical examination, and radiographic studies. The clinician should be astute to the extent of mucosal involvement, depth of invasion, as well as mobility of the vocal folds and arytenoids.
The guiding principles of organ-sparing surgery are to provide oncologically sound outcomes while preserving the sphincteric, respiratory, and phonatory capabilities of the larynx. An attempt should be made to maintain the 3 fundamental functions by preserving at least 1 functional cricoarytenoid unit. In addition, the cricoid cartilage is the only complete cartilaginous ring in the airway, and must be preserved in order to prevent airway compromise.
Bilateral compromise of the cricoarytenoid units or the structural integrity of the cricoid cartilage should preclude organ preservation surgery as an option.
Certain properties of the laryngeal cartilaginous and fibrous framework should be taken into account, particularly in the way they impact tumor growth and extension capabilities ( Fig. 1 , [CR] ). In Brennan and colleagues’ review of the literature, the majority of squamous cell carcinoma (78%) invasion was through direct extension, with only 10% (11 of 107) of cases exhibiting documented involvement via lymphatic spread.
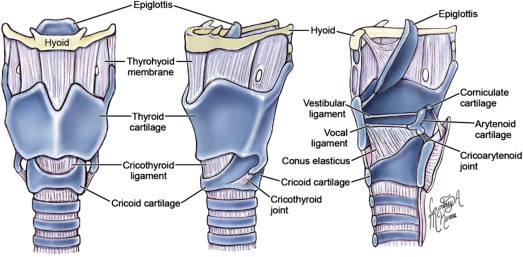
Early glottic lesions may respect the fibroelastic framework of the larynx, whereas larger lesions may utilize the framework for further extension. Laryngeal regions most susceptible to spread are at the anterior angle of the thyroid cartilage and the cricothyroid membrane. Histopathologic studies have shown that tumor spread seems to occur along collagen bundles where the connective tissue membranes attach to the cartilage. As the tumor expands, it causes expansion of the collagen bundles, resulting in a direct pathway for the spread of the lesion through the perichondrium. This subsequently makes the cricothyroid membrane and anterior commissure ligament more susceptible to direct extension of tumor.
Perichondrium may provide a barrier to direct extension of laryngeal tumors. However, once the tumor has compromised this barrier, it may allow for the tumor to spread in a subperichondrial plane behind an intact perichondrium. This may contribute to understaging of laryngeal cancers and inaccurate assessment of thyroid cartilage involvement. Recognizing the latter is critical in directing appropriate management when considering open laryngeal procedures. Direct extension may occur through areas of ossification and osteoclast formation, or areas of high vascularity. Furthermore, thyroid cartilage involvement may occur through areas devoid of perichondrium (eg, Broyles ligament insertion at the anterior commissure) along collagen bundles.
The anterior commissure is an area of epithelial confluence of the anterior vocal folds, covering the posterior aspect of the thyroid cartilage at the midline. Inserted onto the anterior commissure is Broyles ligament, which is a continuation of the vocal ligament. No perichondrium surrounds Broyles ligament, which is connected superiorly with the thyroepiglottic ligament via fibrous extensions. Inferiorly, the anterior commissure is connected to the cricothyroid ligament, a central condensation of the conus elasticus. The dense condensation of fibers that exists in this region forms a barrier to the spread of early glottic lesions, preventing erosion and further superior and inferior extension, as well as extension into the thyroid cartilage. However, in more extensive lesions, the lack of perichondrium in this region, and fibrous connections superior to the thyroepiglottic ligament and inferior to the cricothyroid ligament, allow for these lesions to spread with little resistance. Nevertheless, expanded studies based on the experience gained with transoral approaches suggest that local failures at the anterior commissure have resulted from inadequate surgical exposure and insufficient resection, rather than presumed more aggressive biologic features or deficient barriers at that level. These anatomic considerations are reflected in studies that show increased rates of local failure and recurrence in glottic lesions with anterior commissure involvement.
Clinical or radiographic evidence of anterior commissure involvement should prompt the clinician to appropriate patient counseling when discussing surgical versus nonsurgical options in the management of T1, T2, and select T3 lesions.
Vertical partial laryngectomy
Vertical partial laryngectomies (VPLs) involve a vertical median or paramedian incision through the thyroid cartilage to gain access to the larynx at the glottic level. VPL typically involves resection of 1 or 2 vocal folds, and anterior commissure, with or without partial resection of thyroid cartilage. However, advances in access to the glottis via transoral approaches have resulted in VPL becoming predominantly of historical interest.
Indications include :
- 1.
Large T1 glottic cancers confined to a single cord
- 2.
Small T2 glottic cancer with minimal extension into the supraglottis or subglottis
- 3.
Early glottic lesion precluded from transoral resection due to inadequate exposure
- 4.
Salvage surgery for early glottic recurrence in the setting of failed radiotherapy
Contraindications include :
- 1.
Involvement of the cricoarytenoid joint
- 2.
Thyroid cartilage involvement
- 3.
Extension of the glottic tumor to more than one-third of the contralateral cord
- 4.
Subglottic extension greater than 5 mm
The surgical technique is as follows
- 1.
A transverse skin incision is made
- 2.
Subplatysmal flaps are raised in an inferior and superior direction exposing thyroid cartilage
- 3.
A paramedian or median laryngofissure is made in thyroid cartilage
- 4.
An excision is performed in an anterior–posterior direction to include anterior commissure, ipsilateral vocal fold up to the vocal process, and partial contralateral vocal fold (up to anterior one-third)
- 5.
Superior–inferior extension from the vestibular fold to 5 mm below the vocal fold
Anatomic Basis
VPL surgery is predominantly utilized in resection of early glottic level lesions, with minimal subglottic/supraglottic extension, and no extension into the paraglottic space. Presently, VPL is used in the setting of inadequate visualization via transoral techniques. Paramount to appropriate oncologic margins is absence of extension beyond 5 mm into the subglottis (resection does not extend this far) and absence of vocal fold mobility impairment (indicating paraglottic space extension with thyroarytenoid muscle involvement). Furthermore, failure rates are increased in the setting of anterior commissure involvement due to the increased likelihood of subglottic and thyroid cartilage extension. Intermediate to larger-sized T2 lesions have been reported to have a failure rate of 17% to 40%, with some authors favoring supracricoid resection over VPL.
Horizontal partial laryngectomy
Horizontal partial laryngectomies (HPLs) involve a horizontal incision through or above the thyroid cartilage to gain access to the endolarynx. HPL is classically used for resection of glottic, transglottic, and supraglottic level carcinomas. Principally, there are 3 main variants of horizontal partial laryngectomies, in increasing order of invasiveness: (1) supraglottic partial laryngectomy, (2) supracricoid laryngectomy with cricohyoidoepiglottopexy (SCPL-CHEP), and (3) supracricoid laryngectomy with cricohyoidopexy (SCPL-CHP) ( [CR] ).
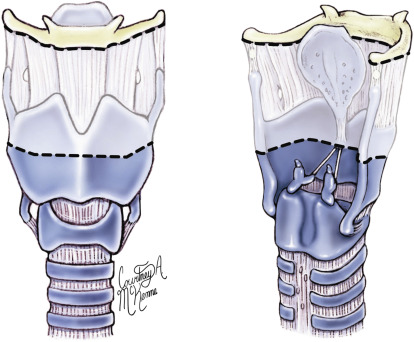
Supraglottic partial laryngectomy
Supraglottic partial laryngectomy involves resection of the pre-epiglottic space, the epiglottis, the vestibular folds, and the upper portion of the thyroid cartilage ( Fig. 2 ). Reconstruction is achieved via a thyrohyoidopexy ( [CR] ).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


