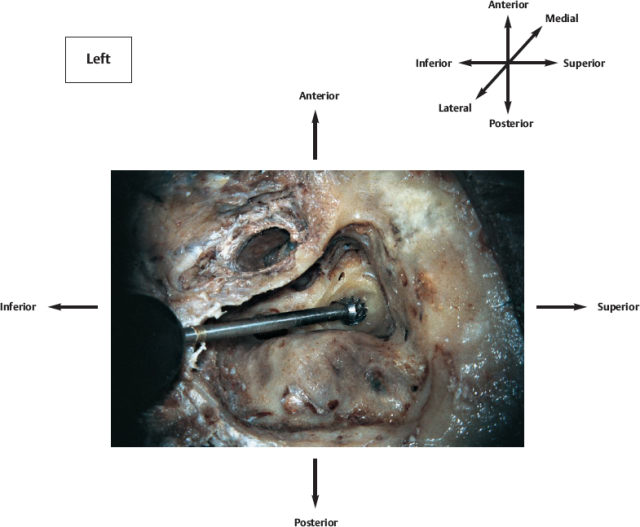
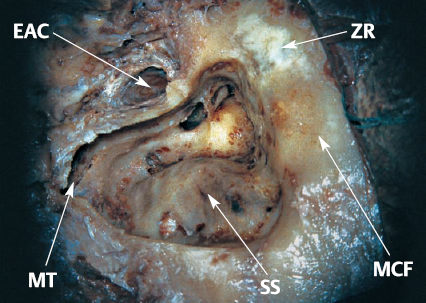
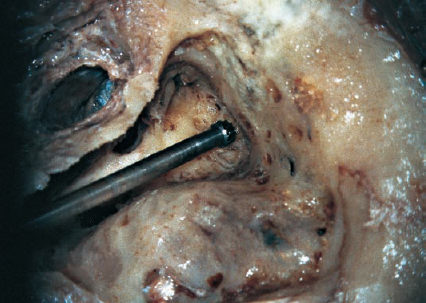
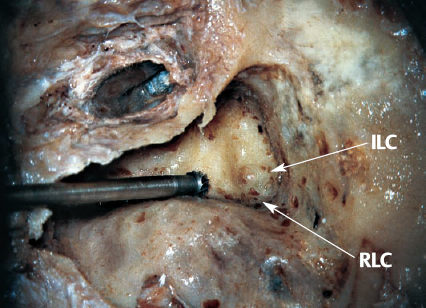
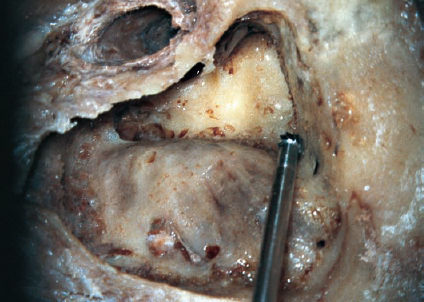
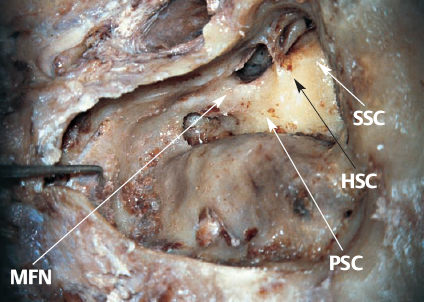
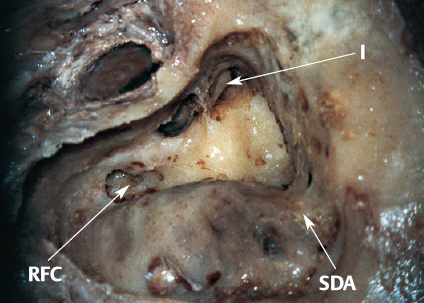
20 Translabyrinthine Approach Following the extended cortical mastoidectomy and exenteration of the posterior part of the labyrinth, exposure of the internal auditory canal, and cerebellopontine angle through the posterior cranial fossa. The main indication of this technique is in acoustic neuroma surgery where the hearing is not of concern. However, it may also be carried out for different neurotologic procedures. A classical cortical mastoidectomy, including posterior tympanotomy has been carried out. The temporal bone is ready for the main steps of the translabyrinthine approach. The limits of the approach are indicated in the figure. EAC: External auditory canal MCF: Middle cranial fossa (dural plate) MT: Mastoid tip SS: Sigmoid sinus (dural plate) ZR: Zygomatic root First, the interlabyrinthine cells are drilled away using a medium-sized cutting burr. Note that the mastoid in this temporal bone is contracted, which means that the sigmoid sinus is located anteriorly and the dura of the middle cranial fossa is located inferiorly. II: 3–4mm cutting burr MIL: Posterior labyrinth (HSC, SSC, PSC) Next, the retrolabyrinthine cells are exenterated using the same cutting burr. In such a contracted mastoid, turning the temporal bone toward the surgeon in the laboratory or tilting the operating table during surgery, would prevent having to work blindly. ILC: Interlabyrinthine cells RLC: Retrolabyrinthine cells Definitions and Tips The sinodural angle is delineated by first using a medium-sized cutting burr, then a diamond burr. The superior petrosal sinus, which runs along the sinodural angle inside the dura, should always be kept in mind and the drilling executed with care. II: 3–4mm cutting and diamond burrs MIL: Sinodural angle The microsurgical instrument is pointing to the exposed digastric ridge. The three semicircular canals are also displayed in this figure, where the next steps of the approach will be carried out. HSC: Horizontal semicircular canal MFN: Mastoid facial nerve PSC: Posterior semicircular canal SSC: Superior semicircular canal Following complete exenteration of the interlabyrinthine, retrolabyrinthine, and retrofacial cells and delineation of the neighboring structures, the cavity has been enlarged from a classical cortical mastoidectomy to an extended cortical mastoidectomy. Note that the facial canal and all the semicircular canals have been skeletonized. I: Incus RFC: Retrofacial cells (removed) SDA: Sinodural angle Definitions and Tips
Definition
Indications
Anatomical Orientation

Surgical Steps
Translabyrinthine Approach
Only gold members can continue reading. Log In or Register to continue

Full access? Get Clinical Tree


