Purpose
To report the corneal thinning during and after corneal cross-linking (CXL).
Design
Prospective, nonrandomized, single-center observational study.
Methods
Thirty patients (30 eyes; 9 female, 21 male; age, 38 ± 12 years) were consecutively scheduled for CXL between January 23 and July 6, 2009. Twenty-four eyes had progressive keratoconus, 2 had pellucid marginal degeneration, 3 eyes had progressive keratectasia after a LASIK operation, and 1 eye had pseudophakic bullous keratopathy. Riboflavin-ultraviolet A (UVA)-induced CXL included the instillation of 0.1% riboflavin drops for 30 minutes followed by riboflavin instillation combined with UVA irradiation for another 30 minutes. Corneal thickness was measured preoperatively, during CXL, and after 1 and 6 months using an ultrasound pachymeter. Changes in the endothelial cell count, corneal steepness, refraction, and visual performance are also given.
Results
On average, the corneas thinned 87 ± 40 μm (range, 37-206 μm; 19% ± 7%) during a 60-minute CXL treatment. In 1 patient, the cornea did not swell, even with hypotonic solution such that CXL would be safe. After 1 month, the corneal thickness was lower than the preoperative thickness, but after 6 months, the corneas had regained their original thicknesses. The endothelial cell count and corneal steepness were unchanged after CXL. The UCVA (uncorrected visual acuity) and BSCVA (best spectacle-corrected visual acuity) were improved 6 months after CXL.
Conclusions
Corneal thickness decreases significantly during CXL, even to a level where the health of the endothelium and cornea is jeopardized. Visual performance is improved 6 months after CXL.
Corneal cross-linking (CXL) is a relatively new technique that induces new collagen cross-links between collagen molecules using the photosensitizer riboflavin (vitamin B2) and ultraviolet A (UVA) light. By modifying the corneal stromal structure, increasing corneal strength and stability, and providing more resistance to enzymatic digestion of the corneal stroma, CXL seems to offer an additional treatment for patients with corneal ectasia, regardless of its cause. However, the technique is not free of complications. In human and rabbit corneas, the cross-linking effect is limited to the anterior 300 μm of the corneal stroma, with a decreasing anterior-posterior pattern that is attributable to the rapid decrease in UVA irradiation across the corneal stroma. Accordingly, thin corneas (<400 μm) are generally unsuitable for CXL treatment. In this study, we measured the corneal thicknesses of eyes undergoing CXL. We found that the corneal thickness is severely decreased during CXL, even to an extent such that it may cause endothelial damage despite an adequate preoperative corneal thickness.
Patients and Methods
Population
Thirty eyes from 30 consecutive patients (9 female, 21 male) were enrolled into the Cornea Service at the Helsinki University Eye Hospital between January 23 and July 6, 2009. Twenty-four of the eyes had progressive keratoconus, 3 eyes had progressive keratectasia after a LASIK operation, 2 eyes presented with pellucid marginal degeneration, and 1 eye had bullous keratopathy after a cataract operation. All of the patients underwent preoperative and postoperative uncorrected visual acuity (UCVA) and best spectacle-corrected visual acuity (BSCVA) assessments, slit-lamp biomicroscopy, Goldmann tonometry, a dilated fundus examination, endothelial biomicroscopy with a noncontact specular microscope (Topcon SP2000P Specular Microscope; Topcon Co, Tokyo, Japan), and corneal topography using an Orbscan IIz anterior segment analysis system (Bausch & Lomb, Rochester, New York, USA). Corneal thickness was evaluated preoperatively and postoperatively and during CXL treatment using an ultrasound pachymeter (Tomey AL-3000; Tomey Co, Nagoya, Japan) by measuring the corneal thickness at its thinnest point (based on topography) 5 times and calculating the average of these readings. The patients were postoperatively examined after 3 days and 1 and 6 months.
Cross-Linking (CXL) Procedure
All of the patients underwent the CXL procedure on a day-surgery basis. Thirty minutes before CXL, pain medication (paracetamol, 1 g; Orion, Espoo, Finland) was administered orally. CXL was conducted under sterile conditions in an operating theater. After topical anesthesia (Minims tetracaine hydrochloride, 1% w/vol; Chauvin Pharmaceuticals Ltd, Essex, United Kingdom), the central corneal thickness was recorded using an ultrasound pachymeter, as described above. A lid speculum was applied, and the cornea was rinsed with saline. The central corneal epithelium was scraped with a single-use hockey-stick blade (Grieshaber; Alcon, Schaffhausen, Switzerland) across an 8- to 9-mm-diameter area, and the central thickness was recorded again. The lid speculum was removed. Isotonic or hypotonic riboflavin (0.1%, Medio-Cross; Medio-Haus Medizinprodukte GmbH, Neudorf, Germany) drops were applied to the cornea every 2 minutes for 30 minutes to saturate the cornea, and the central corneal thickness was recorded at least every 10 minutes using an ultrasound pachymeter. After 30 minutes, a slit-lamp examination using a blue filter ensured the presence of riboflavin in the anterior chamber. The corneal UVA exposure lasted for 30 minutes, during which isotonic or hypotonic riboflavin (0.1%) drops were applied to the cornea every 3 minutes for 30 minutes. The cornea was hydrated using distilled water or hypotonic riboflavin (0.1%) drops if the corneal thickness was <350 μm at any time during the CXL treatment. UVA exposure was performed using a solid-state UV emitter (UV-X System; Peschke Meditrade GmbH, Huenenberg, Switzerland). The device emits light with a wavelength of 370 ± 5 nm, an irradiance of 3 mW/cm 2 , and a light beam diameter of 7.5 mm. A calibrated UV meter (Lutron YK-34UV; PeakTech, Ahrensburg, Germany) was used to verify the irradiance (3.00 ± 0.03 mW/cm 2 ) before the treatment. Fixation during irradiation was achieved by instructing the patient to focus on the light-emitting diode on the UVA emitter. The surgeon’s thorough control ensured the patient’s centration. Topical anesthetics were administered as needed. After 30 minutes of UVA exposure, the cornea was rinsed, and a soft-bandage lens (Polar Lens 75%; Polarlens, Ristiina, Finland) was applied for 3 days. The postoperative medication included 5 mg/mL levofloxacin (Santen, Tampere, Finland) drops 4 times per day for 5 days and lubricant drops (Oculac; Novartis Pharma, Basel, Switzerland) several times per day. The patients also used paracetamol-codeine (Panacod; Sanofi-Aventis, Paris, France) pain medication as needed for the first 2 to 3 days. After re-epithelialization (within 3 days), fluorometholone acetate (0.1%) drops (FML Liquifilm; Allergan Inc, Irvine, California, USA) were used 3 times daily for 14 days and then twice daily for 14 days.
Statistics
Statistical analysis of the paired outcomes was performed using 2-way paired t tests. One-way ANOVA for repeated measures with Bonferroni’s multiple comparison adjustment was used for multiple comparisons. All of the analyses were done with GraphPad Prism (version 4.03) for Windows (GraphPad Software, San Diego, California, USA). A P value of ≤.05 was considered to be statistically significant.
Results
The first 30 patients (9 female, 21 male) who were treated with CXL in the Cornea Service at the Helsinki University Eye Hospital were included in this study. The mean patient age was 38 ± 12 years. The objective of this study was to assess the safety and usefulness of CXL for the treatment of corneal ectasia. Because the most severe threat to corneal fitness posed by CXL treatment is endothelial damage attributable to excessive corneal thinning, we assessed corneal thickness preoperatively, during CXL, and 1 and 6 months after CXL.
Corneal Thickness
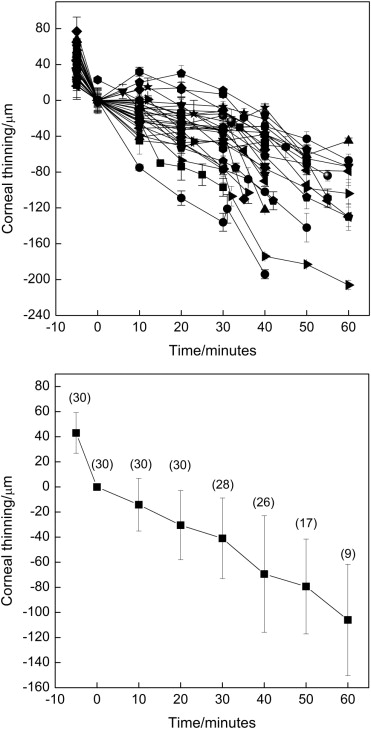
The mean preoperative corneal thickness at the thinnest point was 483 ± 54 μm (range, 371-625 μm), and after epithelial removal, the thickness was reduced to 442 ± 46 μm (range, 348-590 μm). During CXL treatment, the corneal thickness was reduced in all of the patients, and in 24 of 30 eyes (80%), the thickness at any time point was less than 350 μm. This corneal thickness initiated corneal rehydration by either distilled water or hypotonic riboflavin solution. Corneal swelling or rehydration (a corneal thickness of <350 μm at any point during CXL) began 41 ± 12 minutes (range, 20-55 minutes) after the initiation of the treatment. Figure 1 (Top) shows the time-dependent corneal thinning during CXL until corneal swelling (hydration), if needed, was induced in each individual patient. On average, the corneal thickness decreased by 87 ± 40 μm (19% ± 7% of the corneal thickness) during the 60-minute treatment or before the initiation of corneal swelling. The thinning exhibited a 2-phase reduction in thickness. In the first 30 minutes, the thinning occurred much more slowly than in the second 30 minutes ( Figure 1 , Bottom). This can most likely be explained by lid closure in the first 30 minutes, whereas in the last 30 minutes, a lid speculum holds the eyelids open and facilitates water evaporation from the corneal stroma.