Tonsils
Tonsillar hyperplasia and recurrent pharyngotonsillitis are common disorders in children. Tonsillar hyperplasia may cause sleep disorders, disordered breathing, or apnea. Recurrent infections, which are often debilitating on their own, may be associated with complications of streptococcal infection (e.g., rheumatic heart disease, glomerulonephritis, scarlet fever).
19-1 Tonsillectomy (Extracapsular and Intracapsular)
Indications
Removal of the pharyngeal tonsils is indicated to relieve pharyngeal obstruction and to reduce the frequency and severity of pharyngeal infection.
Preoperative Evaluation
The history and physical examination are usually sufficient to determine the need for tonsillectomy. Nasopharyngoscopy may be helpful in cases of smaller appearing tonsils that have a significant inferior extension.
Operative Technique: Extracapsular
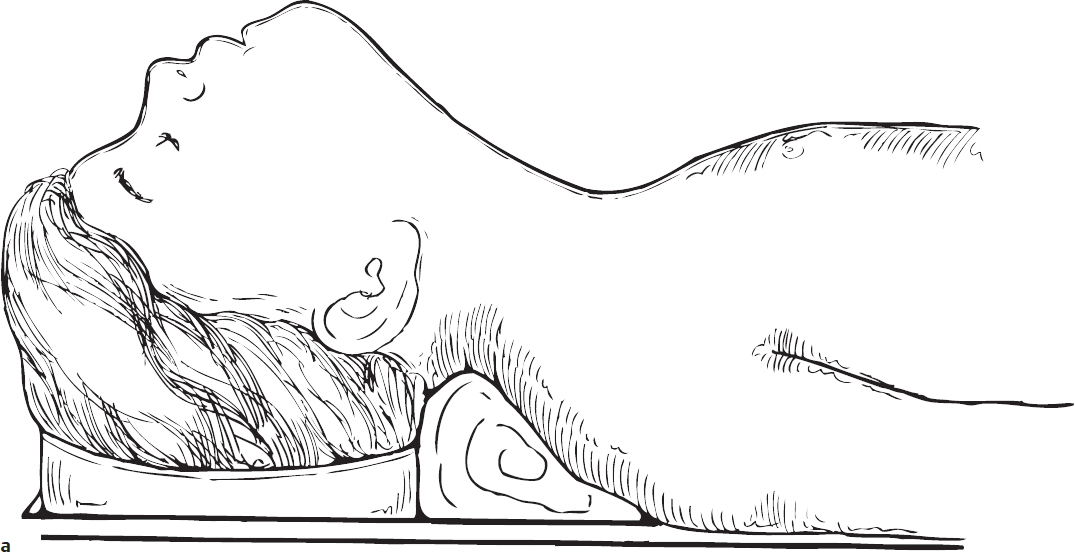
1. Tonsillectomy is usually performed under general anesthesia utilizing an oral RAE tube. A cuffed tube or a throat pack around the tube is suggested to prevent an air leak and to avert the risk of an airway fire. The patient is placed in the Rose position at the end of the operating table. A shoulder roll is placed under the shoulders and the head rests in a doughnut (Fig. 19.1a).
2. A tonsil gag (Crowe-Davis or Dingman) is introduced and opened, keeping the tongue in the midline. The mouth gag is suspended from a Mayo stand. Care is taken not to overextend or hyperflex the neck in patients suspected of having cervical spine abnormality. It is suggested that no shoulder roll be used in a patient with possible C-spine abnormalities and that the mouth gag be supported on the anterior chest wall of the patient with a small roll of towels such that the neck remains in a neutral anatomical position.
3. The posterior and lateral walls of the pharynx are carefully inspected and palpated to detect abnormally positioned vessels.
4. The hard palate is palpated to detect a submucous cleft palate (Fig. 19.1b).
5. The superior pole of the right tonsil is grasped with an Allis clamp, and the mucosal cut on the anterior pillar is outlined with a protected cautery, preserving as much mucosa as possible (Fig. 19.1c,d). The guarded cautery blade prevents inadvertent burns. It is suggested to use cautery settings for this procedure that will both allow dissection of the tissue and achieve hemostasis.
6. The cautery blade can be used for both cutting through the tissue as well as blunt dissection and, after careful dissection, the plane of the tonsillar capsule is located.
7. The tonsil is removed by dissection with the cautery as the tonsil is retracted medially with the Allis clamp (Fig. 19.1e). Larger vessels, when encountered, may need additional cauterization. As the tonsil is removed, the posterior pillar attachment of the tonsil is also incised. The plane of dissection is onto the tonsil capsule and not into the underlying muscle.
8. The attachment of the inferior portion of the pharyngeal tonsil to the lingual tonsil is transected with the cautery (Fig. 19.1f).
9. Residual bleeding vessels are cauterized with a suction cautery while the tonsil fossa is exposed using a hemostat or a Hurd dissector for retraction (Fig. 19.1g).
10. The recessed superior pole of the tonsillar fossa is best visualized using a mirror (Fig. 19.1h).
11. This procedure is repeated on the opposite side.
12. When the tonsillectomy is completed, the mouth gag is released for a brief period along with light massage of the lateral neck and/or the tonsillar fossae; the gag is then reopened to inspect the oral cavity to make sure that there is no further bleeding from vessels that might have been compressed by the mouth gag. The gag is then carefully removed from the oral cavity to avoid accidental extubation of the patient.
Operative Technique: Intracapsular
The intracapsular tonsillectomy, also referred to as a tonsillotomy, can be performed using a microdebrider or a coblation wand. With this technique, 90–95% of the tonsil tissue is removed, starting at the medial aspect of the tonsil and continuing into the tonsil fossa, leaving behind a thin layer of tonsil tissue and the tonsil capsule (Fig. 19.1i). Cauterization of any residual vessels is done as described in steps 9-12 above.
Complications
1. Postoperative hemorrhage
2. Tonsil regrowth