Tongue
The tongue is an active participant in feeding. Restrictions of tongue mobility may interfere with nutrition, growth, and development in the neonate.
20-1 Frenulectomy/Frenulotomy
Introduction
Ankyloglossia is a common cause of feeding problems in neonates. It is a very infrequent cause of articulation problems. Tethering of the tongue can limit its mobility resulting in poor latching and sucking ability in newborns. Severe, thick ankyloglossia may cause pressure against the teeth or trauma to the lingual frenulum itself by rubbing against the lower teeth. The frenulum can get caught in between the lower, central incisors. Tethering of the tongue also limits one’s ability to clean away debris in the gingiva-buccal sulcus and can contribute to dental disease.
Indications
Frenulectomy or frenulotomy is indicated in symptomatic ankyloglossia in newborns or young children.
Preoperative Evaluation
Inspection of the floor of the mouth or frenulum is sufficient. No additional evaluation is required. A speech evaluation may be helpful in the verbal child to determine if the ankyloglossia is contributing to articulation difficulties.
Operative Technique
1. The procedure can be done in the outpatient clinic.
2. The child is held by an assistant. The tongue is elevated with a tongue blade or heart-shaped retractor (Fig. 20.1), and the frenulum is divided sharply with scissors, taking care to stay superior to the submandibular ducts; 1% lidocaine may be applied to the frenulum with a small pledget for mucosal analgesia.
3. Digital pressure with a finger and a sponge is then applied to achieve hemostasis. Oxymetazoline spray can also be applied to the tongue if needed.
Complications
1. Postoperative hemorrhage
2. Submandibular duct injury
3. Recurrence of ankyloglossia
4. Submandibular gland swelling
20-2 Frenuloplasty
Introduction
Once teeth have erupted, the procedure is done under general anesthesia. If the frenulum is very short or thick, a larger horizontal incision through the frenulum is needed. By closing the incision in a vertical direction, the incision site is lengthened, providing further mobility of the tongue.
Indications
Frenuloplasty is indicated for symptomatic severe ankyloglossia.
Preoperative Evaluation
Inspection of the floor of the mouth or frenulum is sufficient. No additional evaluation is required.
Operative Technique
1. Frenuloplasty in children is performed using general anesthesia. This can be done by mask induction, by nasotracheal intubation, or with an oral tracheal tube taped to one side of the mouth.
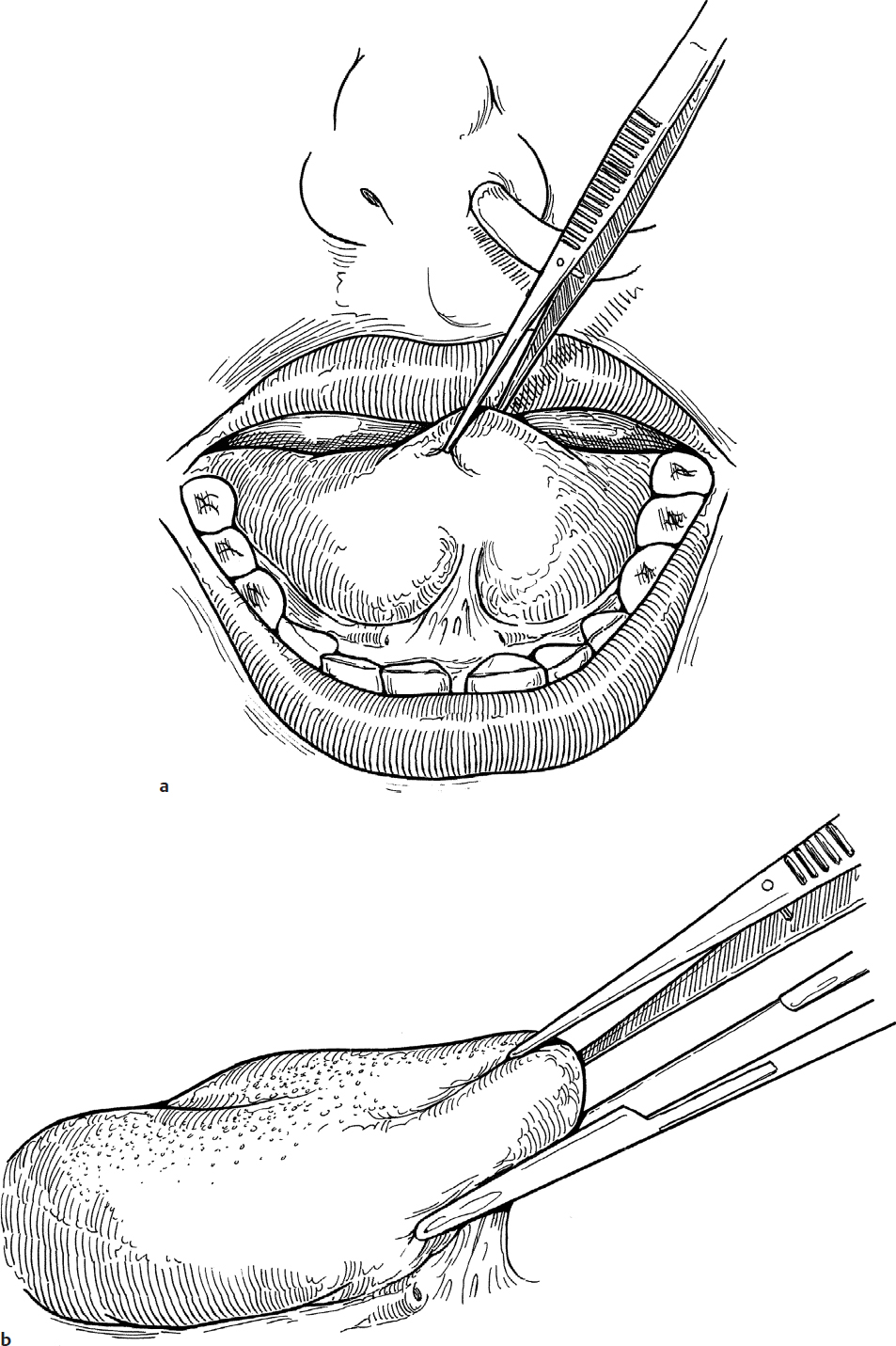
2. The tongue is grasped with toothed forceps and the frenulum is stretched (Fig. 20.2a).
3. The frenulum is crushed with a straight clamp above the submandibular ducts, taking care to avoid injury to the orifices (Fig. 20.2b).
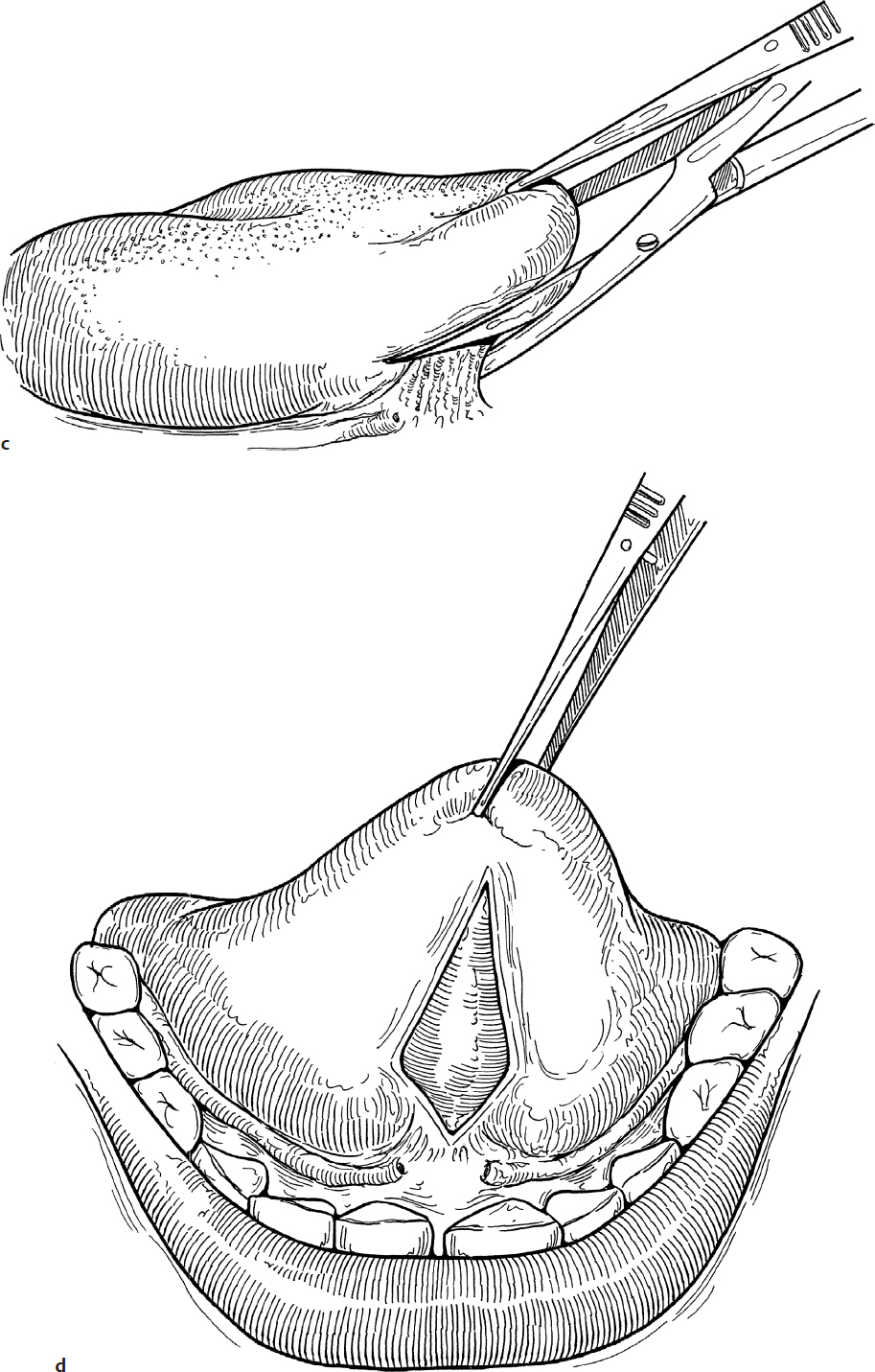
4. The crushed frenulum is cut with scissors up to the base of the sublingual area, releasing the frenulum (Fig. 20.2c).
5. Alternately, the frenulum can be divided with a guarded needle point cautery.
6. This releases the tongue and leaves a mucosal defect on the tongue, extending to the floor of the mouth (Fig. 20.2d).
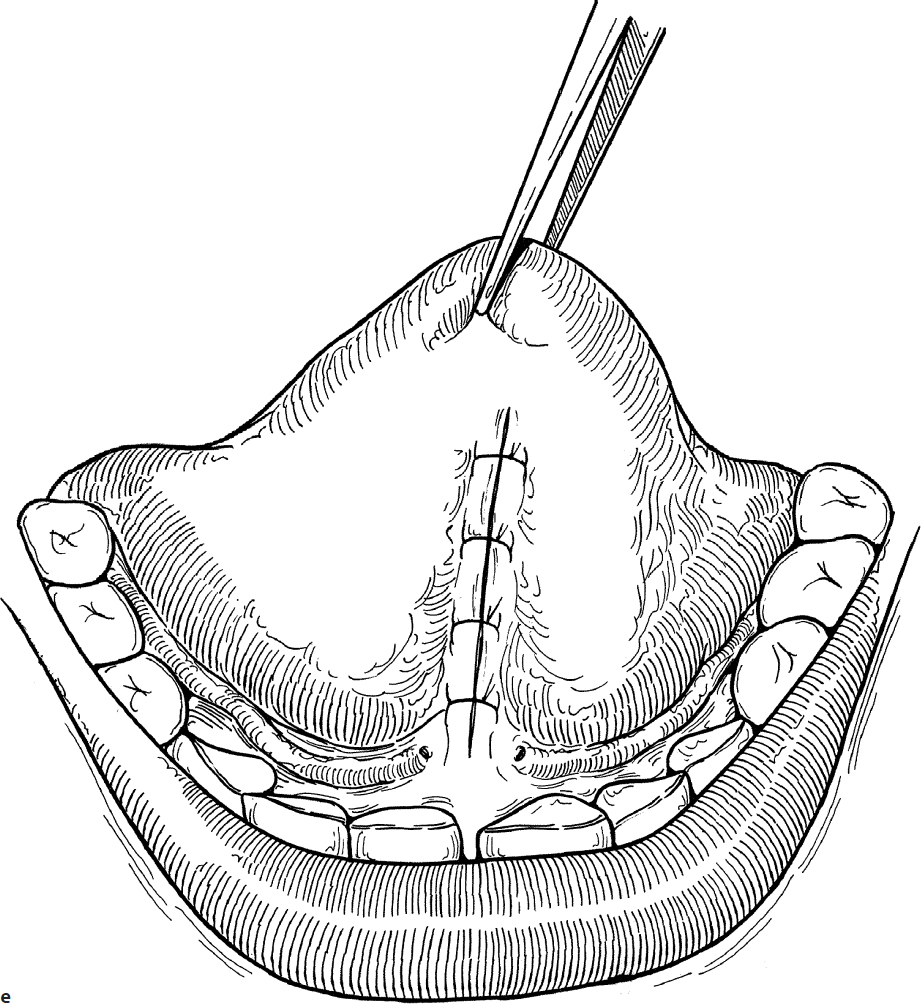
7. Three or four 4-0 interrupted chromic sutures are placed to close the incision on the ventral surface of the tongue (Fig. 20.2e). No sutures are placed in the floor of the mouth because of potential injury to the submandibular ducts and to allow drainage of the intraoral incision site.
8. If the frenulum is thin, suturing may not be needed.
Complications
1. Submandibular duct injury
2. Recurrence of ankyloglossia
3. Submandibular gland swelling
20-3 Excision of Discrete Tongue Lesions
Introduction
Discrete lesions of the tongue such as papillomas, granulomas, and fibromas may present in children. Lingual thyroid can also present on the surface of the tongue or submucosally at the tongue base.
Indications
Suspicious lesions on the anterior third of the tongue require excisional biopsy.
Preoperative Evaluation
Inspection of the anterior tongue lesion is all that is required. No further evaluation is needed. Posterior tongue lesions may require magnetic resonance imaging (MRI) or computed tomography (CT) for complete evaluation. Ultrasound may also be helpful.
Operative Technique
1. Discrete lesions of the tongue are excised using general anesthesia administered through nasotracheal intubation to facilitate intraoral exposure.
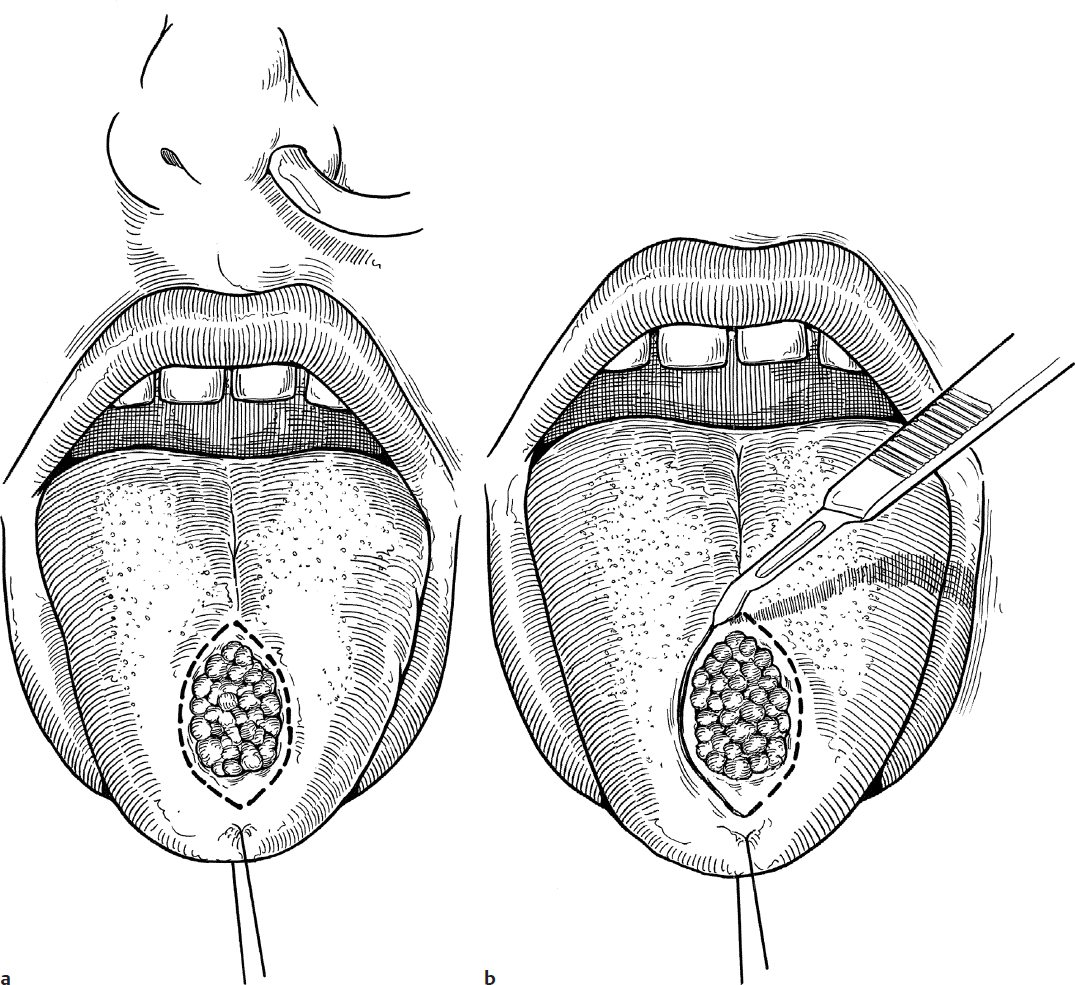
2. A 3-0 silk suture is passed through the anterior portion of the tongue and used for traction (Fig. 20.3a).
3. One percent lidocaine with 1:100,000 epinephrine is injected subcutaneously at the site of the incision to aid in hemostasis.
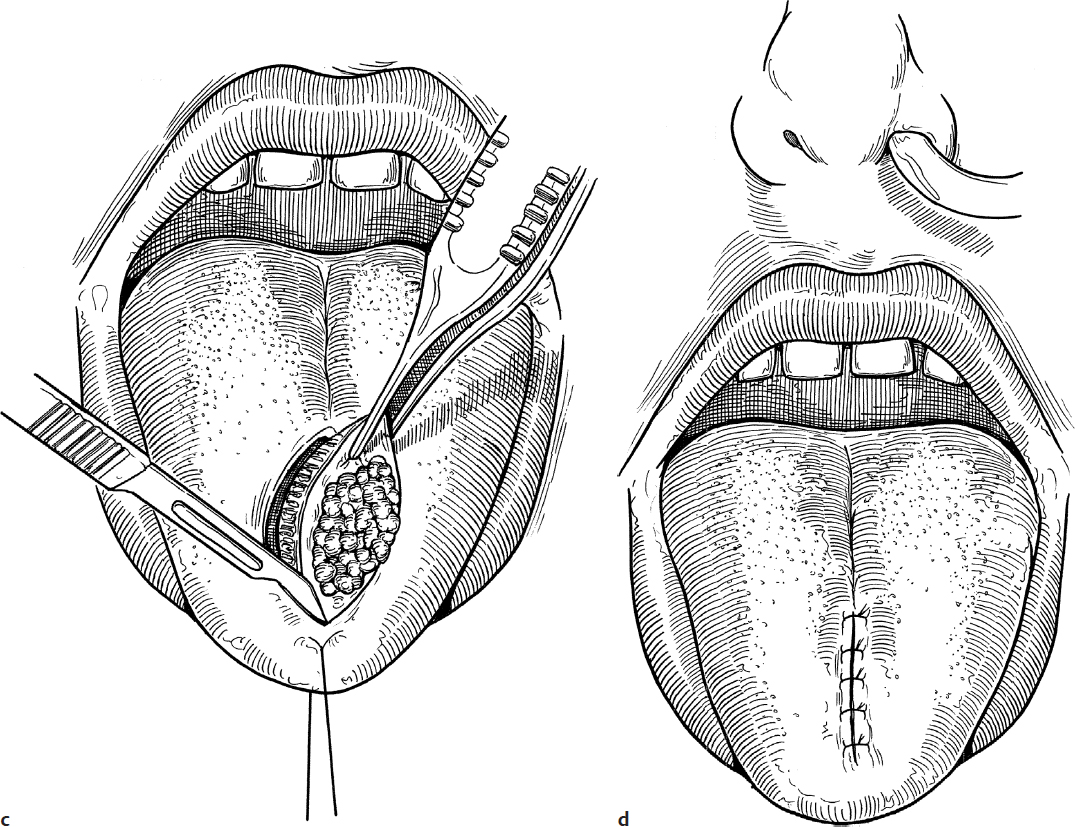
4. The lesion is excised with an elliptical incision through mucosa and into the underlying muscle (Fig. 20.3b,c).
5. The incision is closed with a single layer of 3-0 interrupted chromic suture (Fig. 20.3d).
Complications
1. Wound dehiscence
2. Bleeding
20-4 Excision of Lingual Thyroglossal Duct Cysts
Introduction
Base of tongue masses, such as lingual thyroid tissue or cysts, can present on physical exam or may be diagnosed by CT or MRI.
Indications
Masses within the base of tongue muscle or within the vallecular region at the base of tongue require excisional biopsy.
Preoperative Evaluation
These lesions frequently present with symptoms of dysphagia. CT scanning or MRI evaluation is helpful for masses or cysts within the tongue musculature to delineate depth and extent of the cyst. Preoperative evaluation of presumed lingual thyroid cysts should include an ultrasound of the neck or thyroid scan to confirm the presence of normal thyroid tissue.
Operative Technique
1. Surgery is performed under general anesthesia utilizing a cuffed nasotracheal tube. The patient can be in Rose position with neck hyperextended or in a more neutral position. This latter position is required for a patient with potential C-spine anomalies.
2. Antibiotic coverage is suggested for masses that are within the tongue musculature.
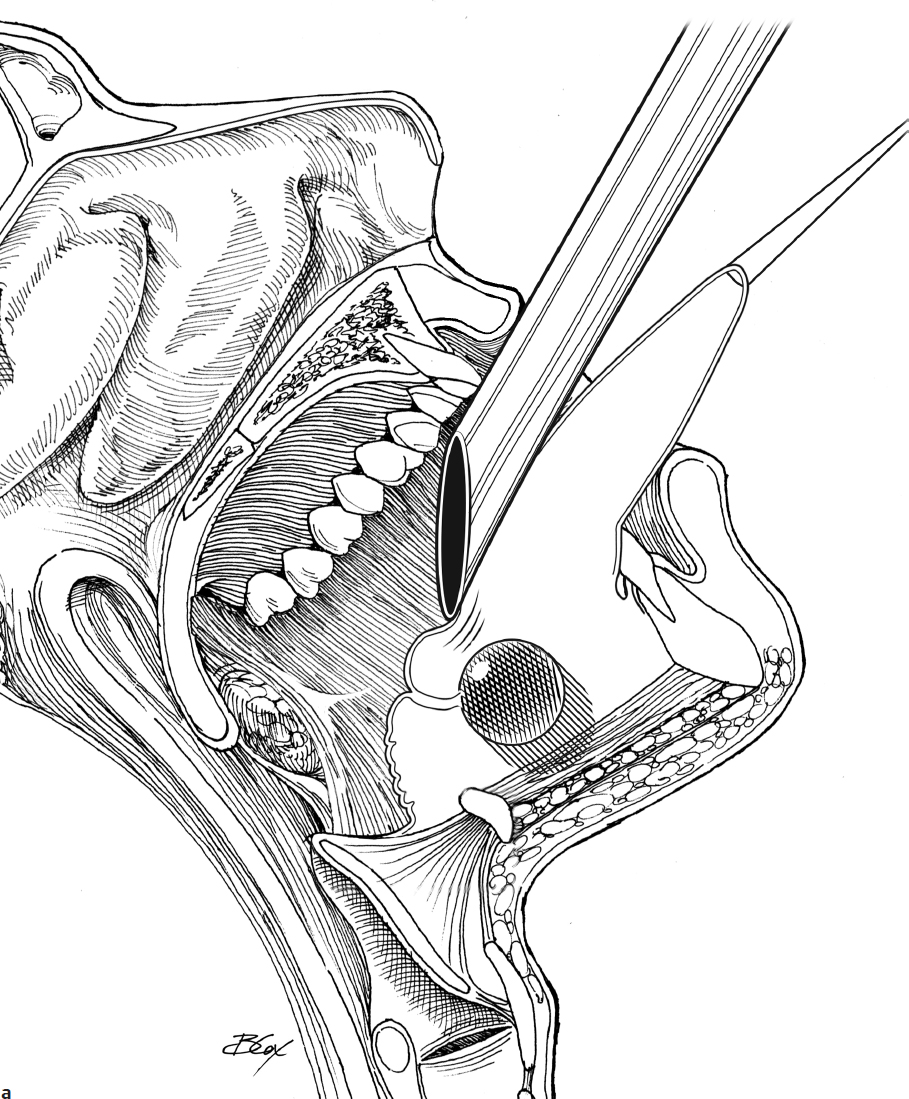
3. A 3-0 silk suture is placed through the anterior tongue tip for retraction purposes.
4. A Lindholm laryngoscope is used to visualize the base of the tongue, and the laryngoscope is suspended from a Mayo stand (Fig. 20.4a).
5. Alternatively, depending on the location of the lesion to be excised, visualization of the appropriate area of the tongue may be done with either a Dingman or Crowe-Davis mouth gag or suspension.
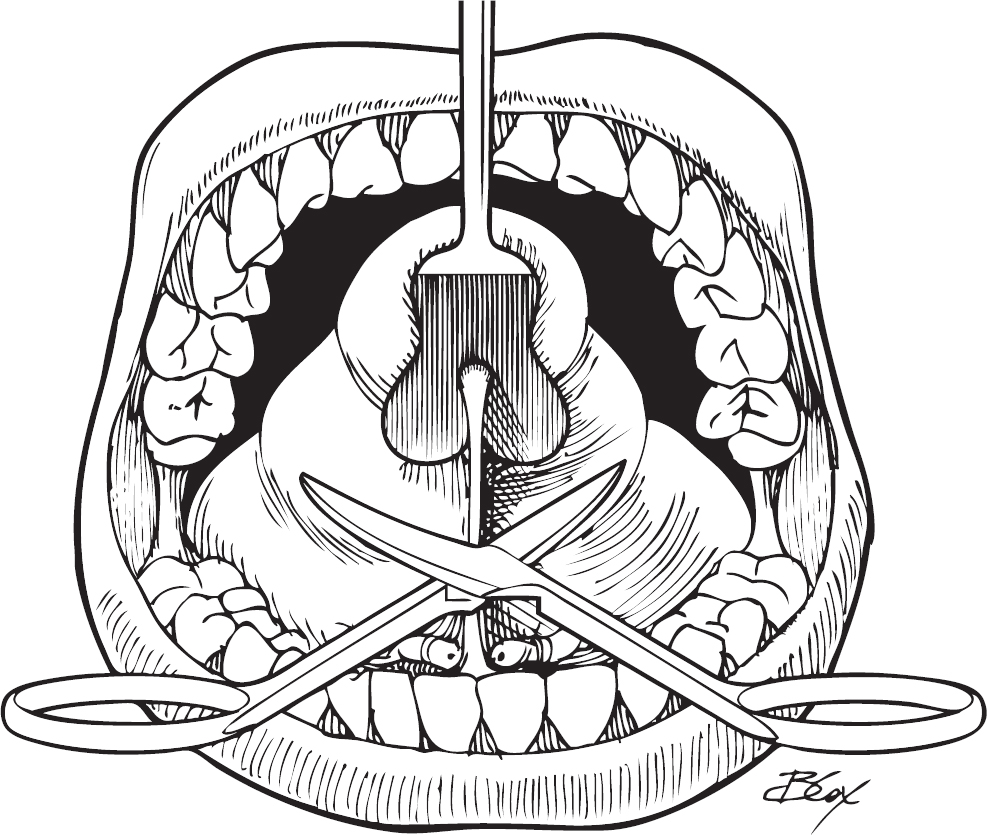
6. One percent lidocaine with 1:100,000 epinephrine is injected submucosally at the site of the incision for hemostasis.
7. Vallecular cysts can be fully excised with sharp and blunt dissection using scissors (Fig. 20.4b) or with a guarded needle point cautery (Fig. 20.4c) with extended hand piece.
8. Intramuscular cysts of the tongue require incision into the tongue base and dissection to locate the cyst wall with further sharp and blunt dissection. The base of the cyst should be tied off in case there is an associated tract.
9. Incision sites are either left open for secondary closure or closed loosely with interrupted Vicryl (Ethicon) or chromic sutures.
Complications
1. Recurrence of cyst
2. Base of tongue infection