Both authors have no conflict of interest and adhere to ethical guidelines.
The reconstructive ladder is a philosophical model used in facial plastic surgery to address cutaneous and soft tissue defects. The reconstructive ladder represents a graduated approach (Fig. 175.1), with closure via secondary intention as the most basic technique and closure with a microvascular free flap as the most complex technique. Tissue expansion falls in the upper middle tier of the reconstructive ladder. It is used when there is not enough adjacent tissue to close a defect primarily or with a local flap.
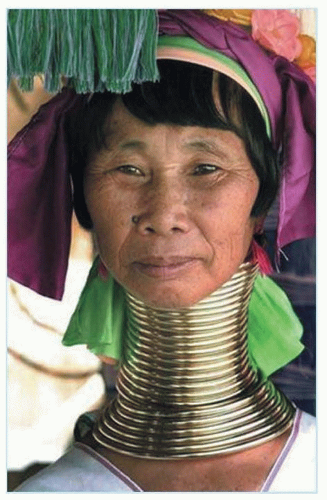
Tissue expansion is a technique used by plastic and reconstructive surgeons to cause the body to grow additional skin, bone, or other tissues. Tissue expansion also occurs naturally in the human body. It can occur as a normal physiologic process—the most classic example is pregnancy, during which uterine and abdominal tissue undergo remarkable expansion and enlargement. Also, it can occur as a pathophysiologic process, such as with large tumors that lead to concurrent expansion of the overlying skin and soft tissue. Examples of tissue expansion can be seen in many cultures. Certain populations have employed forms of tissue expansion to decorate, enhance, or mutilate facial or body structures. The Mursi tribe of Ethiopia incorporates giant decorative plates in the lower lip (Fig. 175.2). The Kayan woman of Myanmar, formerly Burma wears a series of rings around the neck to enhance linear growth (Fig. 175.3). Tissue expansion is also seen in more mainstream culture with the popularity of body art and piercings. Similar to the use of large wooden spools used in the Waorani tribe of Ecuador, the youth counterculture has adopted ear gauges to widen the ear lobe as an expression of body art.
In 1905, Codvilla reported the first use of tissue expansion for medical purposes to lengthen a femur (1). In 1957, Neumann provided the first report of expanding the skin using an inflatable balloon, used in the setting to reconstruct a helical defect (2). Tissue expansion is best known for its use in breast reconstruction. Radovan popularized tissue expansion for postmastectomy breast reconstruction (3). In the 1980s, studies investigating the histologic effects of tissue expansion elucidated the biology and physiology behind this emerging reconstructive technique (4, 5). Argenta reported the first description of tissue expansion in the pediatric population in 1981 (6). Tissue expansion became a widely accepted technique in the 1980s and has continued to be a useful technique in the armamentarium of the reconstructive surgeon.
The advantages and disadvantages of tissue expansion are outlined below (Table 175.1). The ability to bring skin with near-perfect match in color and texture is a significant benefit when compared with skin grafts and pedicled or free flaps, which often transfer tissue that is not similar in texture, thickness, or color. There is also minimal or no donor site morbidity because no secondary defect occurs. Tissue expanders are also able to incorporate tissue with specialized function or adnexal characteristics. For example, tissue expansion in the setting of breast expansion is able to preserve superior sensation in the skin flaps. In the setting of tissue expansion in the scalp for treatment of alopecia, tissue expansion can incorporate hair-bearing flaps. One major disadvantage of tissue expansion is that it does involve multiple surgeries and/or office visits. There is a noticeable visible deformity during the expansion period, which can lead to physical and emotional burdens for the patient.
SKIN BIOMECHANICS AND TYPES OF EXPANSION
Human tissues exhibit dynamic effects when exposed to sustained pressure and expansion. A key understanding of the physical properties of the skin is needed to understand the changes in skin biomechanics during tissue expansion. Tension is a function of the elastic fiber network and varies with location and age. Extensibility is the response of skin to mechanical forces. Viscoelasticity is the function of creep and stress relaxation. Creep is defined as a gain in skin surface area that results when a constant load is applied. In other words, it is the tendency of a solid material to slowly move or deform permanently under the influence of stresses. Stress relaxation is defined as a decrease in the amount of force necessary to maintain a fixed amount of skin stretch over time (7, 8).
Figure 175.1 Reconstructive ladder.
Figure 175.2 Mursi tribe woman of Ethiopia with a giant decorative plate in the lower lip.
Figure 175.3 Kayan woman of Myanmar, formerly Burma with concentric rings around the neck to enhance linear growth.
The concept of creep is essential to understanding tissue expansion. There are different types of creep: biologic and mechanical (Table 175.2). Biologic creep involves permanent changes in the microanatomy of tissue. There is an overall increase in mitotic activity, with resultant net increase in surface area. In contrast, mechanical creep does not exhibit any change in tissue microanatomy. In mechanical creep, there is displacement of fluids and mucopolysaccharide ground substances, microfragmentation of elastic fibers, and alignment of randomly positioned collagen fibers into a more parallel position. There is no overall increase in mitotic activity and thus no net increase in surface area.
Biologic and mechanical creeps correspond to conventional long-term expansion and rapid intraoperative expansion, respectively (Table 175.3). In conventional long-term expansion, biologic creep is the underlying mechanism. It takes weeks to months to achieve and relies on physiologic and histologic changes in the tissue (9, 10). Rapid intraoperative expansion is a more controversial method of achieving tissue expansion. The underlying mechanism that occurs during rapid intraoperative tissue expansion is mechanical creep. There is rapid cyclical stretching of the tissue, which is performed often in a single setting, and results in only mechanical changes in the tissue (10, 11).
TABLE 175.1 ADVANTAGES AND DISADVANTAGES OF TISSUE EXPANSION
Tissue with specialized function or adnexal characteristics
Physical and emotional burden for patient
TABLE 175.2 TYPES OF CREEP
Biologic Creep
Mechanical Creep
Permanent changes in microanatomy
No change in microanatomy
Increase in mitotic activity
Displaces fluid and extracellular substances; collagen fibers realign
Net increase in surface area
No net increase in surface area
PHYSIOLOGY
Maintaining living tissues under tension causes new cells to form and the amount of tissue to increase. An understanding of the skin microanatomy will help elucidate the changes that occur with biologic creep (Fig. 175.3).
The skin is composed of epidermis, dermis, and subcutaneous tissue (hypodermis). The epidermis is the uppermost layer and contains five sublayers (in order from superficial to deep): stratum corneum, stratum lucidum, stratum granulosum, stratum spinosum, and stratum basale. The main cells found in the epidermal layer are Merkel cells, keratinocytes, melanocytes, and Langerhans cells. There are no blood vessels in the epidermis. The dermis is the middle layer and consists of a superficial papillary region and a deep reticular region. The papillary region contains loose areolar connective tissue, and the reticular region contains dense concentrations of collagen, elastic, and reticular fibers. The dermis contains many hair follicles, sweat glands, sebaceous glands, apocrine glands, lymphatics, and blood vessels. The subcutaneous tissue is the deepest layer of the skin and connects the dermis with the underlying bone or muscle—it supplies the underlying tissue with blood vessels and nerves. The main cell types in this layer are fibroblasts, adipocytes, and macrophages.
TABLE 175.3 TYPES OF EXPANSION
Conventional Long-Term Expansion
Rapid Intraoperative Expansion
Takes weeks to months to achieve
Rapid cyclical stretching performed in one setting
Physiologic and histologic changes occur
Mechanical changes only
Relies on biologic creep
Relies on mechanical creep
Well accepted
Controversial
With conventional long-term tissue expansion, biologic creep occurs at all levels of the skin. In the epidermis, there is an increase in mitotic activity. The thickness either stays the same or is slightly increased, and the stratified structure is preserved (10, 12, 13). The changes are temporary, and the microscopic appearance of the skin returns to normal within a year or two after the conclusion of expansion. In the dermis, there is significant thinning of approximately 30% to 50% (10, 14, 15). Of note, however, the basal layer actually thickens. There is increased metabolic activity in the fibroblasts and melanocytes with enhanced collagen synthesis and melanin production, respectively. The number of hair follicles and the pattern of hair growth remain the same, but the density of hair follicles decreases. Individual follicles may be separated by a factor of two without producing noticeable hair thinning. Given normal hair density, the scalp can be expanded by two to three times its original surface area before a change in hair amount is evident. In the subcutaneous tissue, adipose tissue thins approximately 50% with loss of adipocytes (14, 15). There is also some muscle thinning and atrophy (15
Only gold members can continue reading. Log In or Register to continue