7
Tinnitus-Related Insomnia Treatment
The term insomnia covers a range of sleep-related complaints including sleep of insufficient duration, quality, or effectiveness. Like tinnitus, insomnia is very prevalent in the general population (Shapiro and Dement, 1993). Arguably, sleep disturbance is the single most important aspect of tinnitus complaint among adults (McKenna, 2000) and among children (Gabriels, 1995; Kentish et al, 2000). There is evidence that when associated with sleep problems the experience of tinnitus is more distressing (Axelsson and Ringdahl, 1989; Folmer and Griest, 2000; Hallam, 1996; Scott et al, 1990). There is an obvious need to address the issue of tinnitus-related insomnia and its management, but to date few articles have had this subject as a central focus (McKenna, 2000).
The Cognitive Behavioral Model Applied to Tinnitus and Insomnia
There are strong arguments against pharmacological treatment of insomnia (Espie et al, 2001), and psychological management is increasingly recognized as the treatment of choice. The authors facilitated a psychoeducational group for people with tinnitus and sleep problems. It was based on the cognitive-behavioral model, which focuses on the interactions between our environment, thoughts (or cognitions), emotions, behavior, and physical reactions (Greenberger and Padesky, 1995).
Applying the cognitive-behavioral model to tinnitus suggests that the thoughts people have about their tinnitus, rather than the tinnitus per se, determine their level of distress. Thinking of tinnitus as “just a noise” that will not result in physical or emotional harm is unlikely to lead to distress. Conversely, construing tinnitus as a threatening and unmanageable condition will almost certainly lead to distress and greater difficulty in coping with it The behavioral component of the cognitive-behavioral model suggests that the way a person behaves also influences well-being; a person may do things that exacerbate distress, or avoid doing things that alleviate the problem.
The cognitive-behavioral model has also been applied to insomnia (Harvey, 2002a). It has been suggested that people with insomnia suffer from excessive negative thoughts both while trying to go to sleep and during the day and that as a consequence they change the way they behave. The negative thoughts and changed behavior lead to increased arousal, making sleep less likely, and so a vicious cycle is established. Cognitive and behavioral interventions have been found to be helpful in the management of insomnia (e.g., Espie et al, 2001; Harvey et al, 2002; Morin et al, 1999, 2000). Many studies have pointed to the benefits of a cognitive-behavioral approach in tinnitus management (Andersson and Lyttkens, 1999; Henry and Wilson, 1999; Jakes et al, 1986, 1992; Sweetow, 1989). Unfortunately, these studies have shown little benefit on the insomnia component of tinnitus complaint (see McKenna, 2000, for a review). The interventions used, however, rarely if ever focused specifically on insomnia. This has been the inspiration for the authors’ decision to facilitate group therapy focusing specifically on sleep difficulties in tinnitus patients.
It is our view that tinnitus is not a specific sleep antagonist. Rather, the cognitive-behavioral model of insomnia can be applied to the person with tinnitus who suffers from poor sleep. Our hypothesis is that anxiety associated with tinnitus, and with poor sleep, leads to insomnia. A vicious cycle of anxiety, tinnitus, and poor sleep is established. It is common for anxiety about either the tinnitus or poor sleep to assume dominance, and there may be variation in the extent to which each component of the anxiety is present. Many, but by no means all, of our patients have some previous history of sleep difficulties. Our suggestion, based on clinical observation, is as follows: (1) A person may become aware of tinnitus when trying to sleep, or go back to sleep, because the presleep period, with its few other distractions and low levels of ambient noise, offers an opportunity to focus on tinnitus. (2) This leads to unhelpful cognitions about tinnitus and to changes in behavior (e.g., delaying going to bed where tinnitus is more intrusive, drinking alcohol, and checking tinnitus), increased arousal, and distress. (3) This anxiety leads to poor sleep. (4) The sleep difficulties give rise to anxiety again in the form of unhelpful cognitions about sleep, to changed behavior, and to increased arousal and distress. (5) This anxiety maintains the insomnia and leads to greater awareness of tinnitus. (6) Poor sleep maintains the environment that fosters continued awareness of tinnitus (Fig. 7–1). We envisage the process as akin to the “hot cross bun” cognitive-behavioral model of emotional problems described by Greenberger and Padesky (1995) and Williams (2001). We recognize that many of our patients suffer from significant levels of depression, but it is our observation that anxiety processes are the key factors in determining our patients’ poor sleep; it may be that the anxiety represents an aspect of depression in many cases.
Group Therapy for Tinnitus-Related Insomnia
In our clinic we offer both group therapy and individual therapy for insomnia. The focus of this chapter is a description of our group therapy approach for adults with this problem. Individual therapy does not differ fundamentally from the group therapy approach, although it can permit a greater flexibility for people whose problems are multifactorial or who, for some reason, do not meet our group therapy selection criteria. Once the group has commenced, there is no opportunity for others to join the sessions. A new member entering after the first few sessions will gain little benefit because the content of the sessions builds on the knowledge gained in previous sessions. A closed group can enable cohesion to build between group members and may engender a feeling of trust and confidence in the group, enabling members to speak more freely. Individuals in the group have the advantages of meeting and listening to others who are in a similar situation, which can normalize a person’s experiences and reduce anxiety. Patients also can serve as role models for each other. A group milieu may reduce any tendency for patients to dispute the therapist’s ability to understand or help because the therapist does not have tinnitus. Such assumed differences can become barriers to the therapeutic process. From a service perspective, group therapy can be cost effective and may result in more patients receiving the required treatment. Nonetheless, care needs to be taken that the group setting does not lead to disadvantages. Jakes et al (1992) suggested that observing other group members improving may elicit helplessness and envy in some people, or confirm to a patient that his or her problems are unique and therefore much harder to address. In addition, the group environment may result in reinforcement of each others’ negative opinions. It is our practice to use two therapists in each group to help safeguard against such difficulties.
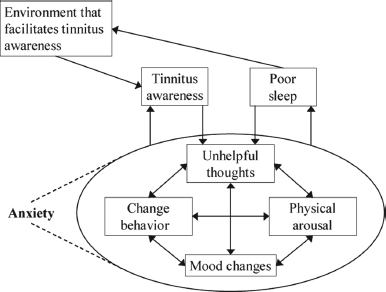
Figure 7–1 A clinical cognitive-behavioral model of tinnitus-related insomnia.
Patient Selection Criteria and Definitions
The problems of insomnia include difficulty falling asleep (initial or early insomnia), waking in the middle of the night and having difficulty returning to sleep (middle insomnia), and waking too early in the morning (terminal or late insomnia). Problems with the quality of sleep translate into complaints of sleep being light, broken, or restless, and not being restorative or refreshing. Complaints about associated daytime problems such as tiredness or sleepiness, mood disturbance, and poor performance are also common.
The quantity of sleep a person gets is not an accurate guide to whether sleep will be regarded as problematic. Some of our patients complain of poor sleep while reporting that they get 8 or more hours of sleep a night; others manage well on little sleep. Subjective complaint about sleep is therefore a key factor in the clinical consideration of sleep problems. To obtain some measure of objectivity, we follow guidelines that are set out in the insomnia literature. We regard sleep as problematic if there is a delay in getting to sleep, or in getting back to sleep in the middle of the night, of at least 30 minutes, or if the total time awake in the middle of the night is 45 minutes, or if the person obtains a total of less than 61 hours sleep (Morin, 1993). These difficulties should occur at least 3 nights a week. In practice many of our patients complain of daytime problems due to insomnia, but we do not regard such complaints as necessary for inclusion in our sleep management program. Sticking to criteria that are rigidly based on time or frequency alone can be problematic. Considerable variability in sleep patterns is seen not only in the general population but also in people complaining of insomnia, and the unpredictability of sleep may be as much a feature of insomnia as a lack of sleep. The importance of complaints about insomnia is therefore often a matter of clinical judgment. Nonetheless, adherence to the time and frequency criteria results in greater homogeneity in the group and avoids the inclusion of people with problems that others regard as implausible.
Another important criterion in our selection process is the establishment that the insomnia is related to the person’s tinnitus. Insomnia, like tinnitus, is a symptom rather than a single disorder, and it can occur for a variety of reasons. Dement and Vaughan (1999) list disruption of the circadian rhythm and psychological disorder as among the main causes of persistent insomnia. Both of these problems are commonly reported by our sleep-disturbed tinnitus patients. Provided the psychological disorder is related to the patient’s struggle with tinnitus or the circadian rhythm disturbance is a result of, say, their inappropriate efforts to deal with their insomnia, rather than due to something like shift work, then such patients are included in our group. Restless legs syndrome, periodic limb movement disorder, gastroesophageal reflux, and fibrositis syndrome or other pain states are also possible reasons for persistent insomnia (Dement and Vaughan, 1999). Breathing disorders are also a common cause of insomnia (Williams, 1996), and it is possible for some medications to disturb sleep by producing arousal or by disturbing the phases of sleep (Idzikowski and Shapiro, 1993). Alcohol and illicit drug abuse also can lead to sleep disturbance. We suggest that therapists bear these things in mind when assessing people complaining of tinnitus-related insomnia and if necessary refer the person on appropriately.
Our sleep management program employs psychological rather than pharmacological treatment; however, many of our patients are already taking hypnotics or other psychotropic medication that affects sleep. We request that patients do not alter their medication during the program, unless there is a clear indication that they are taking the medicine inadvertently improperly, or unless a reduction in dose is established as a specific therapeutic goal. In such cases reference is made to the prescribing physician. We do not include people who are significantly abusing alcohol. Many of our patients, however, use alcohol as a sleeping agent, and inclusion or exclusion from our program is dependent on whether the primary problem is the insomnia or the alcohol use. To obtain some homogeneity, we restrict membership of the group to the adult population, (i.e., 18–65 years of age). Older adults are seen on an individual basis.
Assessment
QUESTIONNAIRE MEASURES
Several questionnaire measures are used in the evaluation of our therapy. They are administered 1 month before the start of the therapy, at the start of the therapy, at the end of the therapy, and at a 4-month follow-up. The second edition of the Beck Depression Inventory (BDI-II; Beck et al, 1996) and the Beck Anxiety Inventory (BAI; Beck and Steer, 1990) are used as measures of emotional state, the Tinnitus Questionnaire (TQ; Hallam, 1996) as a measure of tinnitus complaint, and the Pittsburgh Sleep Quality Index (PSQI; Buysse et al, 1989) as one measure of sleep. The PSQI assesses sleep quality during the previous month in terms of seven components: subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleeping medications, and daytime functioning. The seven component scores are then summed to yield a global PSQI score. A disadvantage is that it involves retrospective and somewhat global judgments about sleep that may be subject to reporting biases. An advantage of the PSQI is that it assesses sleep across a range of dimensions, has a high specificity, and is easily administered.
SLEEP DIARY
Sleep diaries used on a nightly basis are the most sensitive self-report instruments for assessing insomnia. They are useful in providing information about the person’s sleep habits and about the areas that require therapeutic intervention. A diary also provides a measure of progress. The diary should ask the person to record information about the time of going to bed, the time when the lights are turned out (i.e., the point at which an attempt is first made to sleep), the number of times the person wakes during the night, the amount of time the person is awake during the night, and the times of final waking and rising. From this the total time in bed and the total sleep time can be derived and a measure of sleep efficiency (the total sleep time expressed as a percentage of total time in bed) calculated. It is also useful to include a measure of sleep quality; this can be done using a 10-point numerical scale, where 0 equals very poor quality sleep and 10 equals very good sleep. Similar scales can be used to assess nightly tinnitus annoyance and daytime functioning. An example of a sleep diary used in tinnitus management is given by McKenna (2000). It is our practice to summarize key aspects of the diary data in graph form. The data chosen depend on the individual patient’s presentation, but typically time in bed and time asleep, or time asleep and quality of sleep, are chosen. The graphs are updated as each new diary is presented and are provided to the patients as a source of feedback. Summary data in terms of mean values can be calculated for final evaluations.
SLEEP NARRATIVE
Patients are asked to give an account of their sleep and sleep-related behavior for a typical 24-hour period. They are asked to describe their preparations for bed. Patients’ bedtime and activity prior to lights out (e.g., reading in bed, watching television in bed) are noted. Patients are asked about their presleep experiences (e.g., checking tinnitus, worrying about the next day), the length of sleep, the timing and duration of any awakenings, what they do during awakenings, final waking times and rising times, and daytime activity, including any naps and any other activity that relates to sleep (e.g., exercise to tire the person out). The story is taken up to the time of preparing for bed the next night. This account highlights the areas in need of intervention; for example, intrusive ruminations and long delay in initial sleep onset and sleeping late in the day.
Group Structure
Our groups comprise 8 to 10 patients. This number of participants allows time to address individual problems within the group, to prevent the quieter members from feeling overwhelmed, and to help the group feel contained. The group runs for 2 hours every 2 weeks. There are eight sessions and one follow-up session at 4 months. The group sessions begin with individual members introducing themselves and giving a brief account of their experience of tinnitus and sleep problems. At this stage patients often state their individual treatment goals; however, goal setting is returned to following some basic sleep education. The introductions are followed by an educational component informing people about sleep, insomnia, and tinnitus. This is followed by the introduction of relaxation techniques and then by the introduction of the cognitive model. Sleep hygiene strategies are then introduced, and later on other techniques for the control of intrusive cognitions while in bed are described. The information provided is supported by handouts, and the participants are given pen and paper to make notes and thus build up a folder to use as a written summary for future use. Cognitive restructuring, relaxation, and sleep hygiene homework are reviewed in each session.
Treatment Protocol
TINNITUS AND SLEEP EDUCATION
Following the introductions, the program moves on to an educational component. This seeks to inform the group members about the nature of tinnitus and about the nature of sleep and insomnia. The intention is to demystify tinnitus and sleep and to provide a framework against which to normalize some of the patients’ experiences (e.g., frequent awakenings) and within which to set realistic goals.
Information about Tinnitus The information provided about tinnitus is based on the habituation model described by Hallam et al (1984). Emphasis is placed on the ideas that the natural history of tinnitus is one in which most people stop responding to tinnitus with the passage of time, and the majority of people who have tinnitus are not greatly distressed by it. Stress is also placed on the ideas that high levels of arousal (or “tension”) and beliefs about tinnitus impede the process of habituation and that the physical parameters of tinnitus are relatively unimportant.
Information about Sleep and Insomnia The sleep education element is derived from psychological writings within the insomnia literature (e.g., Espie, 1991; Morin, 1993) and in particular from a cognitive-behavioral model of insomnia (Harvey, 2002a). Therapists should acquire some basic knowledge about sleep and insomnia before offering a sleep management program to tinnitus patients. At this stage the information presented is restricted to several points about sleep stages, normal sleep times, and the effects of sleep deprivation.
Normal Sleep Times and Sleep Stages Most people get 7 to 8 hours sleep. There is, however, a considerable range in normal sleep times. We illustrate the point that some people manage well on little sleep by reference to a high-achieving person such as former British prime minister Margaret Thatcher, who famously got only 4 hours of sleep a night. It is a commonly held belief that older people do not need as much sleep as they did when younger. Although older people do tend to get less sleep at night, they also nap more in the daytime, so the total amount of sleep achieved remains relatively stable from middle age to later life (Morin, 1993; Reynolds et al, 1985). An attempt is made to normalize the experiences of the group members by reference to the literature.
Sleep stages—rapid eye movement (REM) sleep and non-REM stages 1 to 4—are described, and the cycle of REM and non-REM sleep throughout the night is outlined. Patients are informed that this cycle takes about 90 minutes to complete but can vary from 70 to 120 minutes; the cycle is repeated four or five times a night in normal young adults. A normal night’s sleep also includes several awakenings. These are usually brief, and many people are unaware of them. For most people the first awakening occurs after 2 or 3 hours of sleep. Awakenings become more common as the hours of sleep increase. The first awakening often represents a point at which the structure of sleep changes, with the periods of REM sleep becoming longer. Clinically, the experience is often described in terms of little really deep sleep after the first awakening. Age-related changes in sleep patterns are described. Older people experience less deep sleep; very deep sleep may be absent altogether in older people, and the number of awakenings increases with age. Young adults commonly experience two awakenings in a normal night’s sleep; older people may experience as many as nine awakenings a night. For many elderly people sleep is experienced as light and fragmented. This information is illustrated by using a histogram representation of sleep stages (McKenna, 2000) and by reference to the experiences of the group members. Many people find it difficult to clearly distinguish sleep from wakefulness. This difficulty may be accounted for by the observation that people may continue to think about things even during periods of light sleep; mental activity is mistaken for wakefulness.
Effects of Insomnia The exact function of sleep remains unclear (Shapiro and Falnigan, 1993), and it is more helpful to consider some of the commonly reported difficulties associated with the lack of sleep rather than to discuss the possible function of sleep. People with insomnia complain of a range of deficits, such as daytime sleepiness, poor concentration and memory, and poor performance on daily tasks. The literature on the effects of insomnia does not lend strong support to the idea that insomnia does lead to these deficits. Individual insomniacs vary in their ability to do tasks, and some research studies have found no difference between insomniacs and people who sleep well on psychological tests (Chambers and Keller, 1993; Mendleson, 1990; Mendelson et al, 1984; Schneider-Helmert, 1987; Seidel et al, 1984; Sugarman et al, 1985). Even the idea that insomnia leads to greater daytime sleepiness has been questioned (e.g., Dement et al, 1982; Stepanski et al, 1988). A review by the American Academy of Sleep Medicine (Sateia et al, 2000) concluded that the negative effects of insomnia seem to be caused as much by the anxiety surrounding it as by the sleep loss per se. A discussion of these points is encouraged, and again an attempt is made to relate patients’ experiences to the evidence in the literature. Patients may be skeptical about these ideas, and knowledge of the literature may be vital for the therapist’s credibility. Notwithstanding this, it is our experience that formulating their problems in terms of the effects of increased arousal is credible to most patients.
Tinnitus and Sleep Patients are asked to consider the fact that tinnitus does not lead inevitably to one or another negative consequence. The varying experiences of the group members are drawn upon to illustrate this. The point is then made with reference to tinnitus and insomnia. The group members are informed that only about half of people attending a tinnitus clinic complain of sleep problems. Emphasis is placed on the idea that tinnitus does not inevitably lead to insomnia. The factors that give rise to, and more importantly that maintain, insomnia are highly likely to be psychological in nature and susceptible to psychological treatment. It is our observation that our patients awaken in the night at about the times predicted from a typical sleep cycle, and it is our contention that tinnitus does not wake people up. Once awake, tinnitus may be the first thing that a person is aware of, and he or she may then remain awake for the reasons previously described. We stress the point that we do not view tinnitus as a specific sleep antagonist.
INDIVIDUAL GOAL SETTING
Formal research programs commonly use sleep-onset latency (i.e., the time taken to fall asleep) as a clinical effectiveness measure (see Espie, 1991, for definitions). When it comes to the individual patient, however, greater care is needed in setting treatment goals. Given the subjective nature of insomnia, it is clearly inadequate to set a standard goal for all patients, even to the extent of suggesting that an increase in the amount of sleep obtained should be the goal. Patients’ aspirations for treatment are highly individualistic, and imposing standard outcome criteria is likely to lead to a sense of failure for both patients and therapists. Many patients do hope for an increase in the number of hours of sleep obtained, but many other, equally valid, goals are expressed by patients. These may include sleep without the aid of alcohol or pills, fewer awakenings or improved sleep efficiency (time asleep as an expression of time in bed), more predictable sleep, better quality sleep, a reduction in daytime deficits, and feeling less anxious or depressed. The therapist must consider the individual goals against what is known about normal sleep and against what is possible within the clinic setting and the time available. For example, a goal of 8 hours of uninterrupted deep sleep for a 60-year-old patient may be unrealistic.
RELAXATION
Patients are given a rationale for relaxation therapy in terms of reducing autonomic nervous system arousal. The reduction of muscle tension provokes a similar reduction in other autonomic subsystems, such as heart rate, respiration, and blood pressure. Elevated levels of arousal decrease the likelihood of initiating sleep, and relaxation therapy increases the chances of sleep. Muscle relaxation also has been found to be effective in reducing intrusive thoughts (Nicassio et al, 1985; Sanavio, 1988). It has been suggested that the experience of tinnitus is related to heightened levels of autonomic arousal (Hallam et al, 1984) and that by reducing the level of autonomic arousal, the intrusiveness of tinnitus may also be reduced. Relaxation therapy has considerable face validity, and it may be that some of the benefit derived from it stems from the sense of control that people commonly report when practicing it. We believe that the provision of a clear rationale may enhance the face validity, thus promoting these nonspecific effects and encouraging compliance. By distinguishing relaxation therapy from other activities commonly thought to be “relaxing” (e.g., watching television, reading a novel), the rationale may also reduce these alternative, possibly arousing behaviors. Muscle relaxation exercises are taught in the group, and patients are given recorded relaxation instructions and asked to practice daily.
COGNITIVE THERAPY
The cognitive therapy element focuses on the process of cognitive restructuring. The initial aim of this intervention is to help people understand the relationship between thoughts, emotions, behavior, and bodily sensations. This is achieved by using simple illustrations that demonstrate the link between thoughts and emotions; for example, a friend does not say hello because (1) he is ignoring you, resulting in emotional upset, or (2) he does not see you, resulting in a less distressing emotional state. Once this basic relationship is understood, the point is reiterated with reference to the way unhelpful thoughts about tinnitus and poor sleep contribute to a cycle of distress, increased tinnitus perception, and poor sleep. The patients are asked to think of ways in which their own thoughts contribute to their experience of distress. Initially, the therapist may help by pointing out the thoughts that patients have expressed when relating their history and if need be may help patients in other ways, such as the use of imagery, to access their thoughts. The process of cognitive distortion, wherein thoughts acquire an overly negative bias, is also described and illustrated. The patients are asked to monitor their emotions and thoughts using diaries as a homework task (Greenberger and Padesky, 1995). This helps to consolidate the information learned in the session and encourages group members to begin to recognize their unhelpful thoughts. The next step is to help people begin to reevaluate these unhelpful thoughts. The role of the therapist is to help patients consider alternative and more helpful thoughts about their situation. There are many questions people can ask themselves in an attempt to consider a different perspective about a situation; for example, What’s the evidence for my thoughts? (very often it is scarce) and Is my thought fact, or is there another way to think about this? (see Greenberger and Padesky, 1995). Once the conviction in the initial thought is weakened, the person is encouraged to think about another way of viewing the situation. For example, rather than thinking I’ll never get to sleep and won’t be able to do anything at work tomorrow, it may be more helpful to think I’ve never had a night when I haven’t slept at all, and I’ve always been able to do something at work even when I’ve been very tired. It is important that these new thoughts and beliefs are tested, and work done outside the group is reviewed within the session. For example, with the above situation, the person may be encouraged to record what he or she does at work. This will help to provide evidence against the biased belief that the person will not be able to do anything and collect evidence in support of the new belief.
VIDEO MODELING
There is evidence that seeing other people cope with a problem can be therapeutic for patients with some psychological problems. The present authors are not aware of any studies that have formally employed coping models in tinnitus management, but Davies and colleagues (1995) postulate that improvements in tinnitus patients undergoing group therapy may be due to the modeling seen in group environments. We therefore show recorded interviews with past patients who had a history of considerable tinnitus-related suffering, including insomnia, but who are now coping well following psychological treatment. In our experience tinnitus patients hear that others cope with tinnitus, but they rarely encounter such coping models. Our intention is to provide evidence that tinnitus and insomnia can be managed and to provide a model that the patients can emulate.
SLEEP HYGIENE
As the cognitive model suggests, thoughts and feelings influence people’s behavior. When people have difficulty sleeping, they do things that they believe will help them sleep. Such strategies include taking medication or drinking alcohol, avoiding going to bed, remaining in bed for long periods of time, and watching television in the bedroom. These strategies may offer short-term benefits, but in the long term they may perpetuate the insomnia (Spielman and Anderson, 1999). As long as the person continues to attribute sleep difficulties to the tinnitus rather than to these behaviors, he or she will unwittingly reduce the chances of sleep, and so a cycle is established. Helping the person with insomnia to gain insight into this cycle is the first intervention step. Once the group members have begun to question some of their behaviors, the next step is to discuss sleep hygiene and the behavioral changes they can begin to make to promote sleep. Sleep hygiene interventions must be considered for all people who have poor sleep because even if poor sleep hygiene is not the primary cause of sleep disturbance, it may be a secondary factor that is playing a role in maintaining sleep problems (Spielman and Anderson, 1999).
Alcohol Alcohol may help to induce sleep, but it can also cause sleep disruption throughout the night, especially the second half. The result is early morning wakening. Patients are encouraged to avoid using alcohol as a sleep or relaxation aid.
Caffeine Although it is widely known that caffeine is a stimulant, many people drink tea or coffee before going to bed or if they wake in the night. People are advised to reduce their caffeine intake slowly, to avoid it in the evenings, and to be aware that it is present in a range of foods and drinks (e.g., chocolate, cola drinks).
Nicotine People often have a cigarette before bed or when they wake up in the night. As with alcohol, they may be viewing cigarettes as a means of relaxation. People are advised about the physiological stimulating effect of nicotine and advised to reduce and carefully regulate their intake.
Food Hunger can result in difficulty initiating sleep, but so too can a heavy meal near bedtime. It is important to gain a balance between going to bed hungry or with a full stomach. People are advised not to eat while awake in the night.
Evening Routine People are advised to have a prebedtime routine to help them and their body recognize that it is time to slow down, relax, and sleep. The routine can be very individual, and some of the sleep hygiene can be incorporated. It is helpful to discuss with people their plans for a new routine and to caution against potentially unhelpful behaviors. For example, people often think that a bath close to bedtime will help them to relax. Because of the changes in body temperature, however, it is more helpful to bathe about an hour before bedtime.
Exercise Regular exercise helps well-being and promotes sleep. During and for some time following exercise, however, the body is in an increased level of arousal. It is therefore advisable to engage in regular exercise but not just before going to bed.
The Bedroom and Use of Sound Activities in the bedroom other than sleep result in an association between these activities and the bedroom, thus lessening the association between the bedroom and sleep. People are advised to use the bedroom only for sleeping and sex. If they wish to watch television or read a book, for example, then it is best to do so in another room. Many patients use sound in the bedroom to alleviate their tinnitus. We discourage the use of radios or televisions for this purpose because of their potentially arousing properties, and instead suggest that people use other sources of sound such as commercially available noise generators. If, however, a radio is all that is available, we suggest that it is set to a nonstimulating program at a volume that prohibits hearing what is being said, or better still, to have it out of tune so a noise similar to white noise can be heard. We suggest that if sound is used it be maintained in the bedroom on a 24-hour basis so that it quickly becomes part of the bedroom environment, and any arousing effects are minimized. We discourage the use of sound to completely mask tinnitus because this is considered counterproductive for the habituation process.
Clock Watching For people who have sleep problems, looking at the clock during the night may serve to increase anxiety or dread, decreasing the chances of sleep. The best strategy is not to have a clock in the bedroom, or to turn the clock away if an alarm is needed.
Time in Bed There is a tendency for people who have sleep problems to spend long periods of time in bed in an attempt to compensate for the poor sleep. People are encouraged to spend no more time in bed than absolutely necessary to avoid associating bed with wakefulness and triggering a cycle of unhelpful cognitions and unpleasant emotions, thereby reducing the chances of sleep. It is suggested that people wait until they are feeling tired before going to bed. If they are unable to go to sleep or go back to sleep, it is suggested that after ∼20 minutes they get up, leave the bedroom, and do something restful, avoiding any physiological or psychological stimulation. Once they feel sleepy, they should return to bed; if they are not asleep after another 20 minutes, the routine should be repeated. It is also suggested that people anchor the wake-up time to a regular time (even on weekends). This can be difficult to do, especially when someone has obtained only a small amount of sleep by the wake-up time, but it is crucial to maintain a helpful sleep–wake cycle. Sleeping during the day is discouraged for the same reason but also because it can be a type of safety behavior that prevents the person’s anxieties about poor sleep being challenged and disproved. If a person feels sleepy in the day, he or she should do something that is not conducive to sleep, such as going for a walk.
Worry Time The role of unhelpful cognitions about sleep has been discussed. This can also be applied to other worries in the person’s life. As we are all aware, it tends to be the nighttime when our worries come into and remain in the forefront of our thoughts. Although this may not be helpful for everyone, a suggestion can be to allow a “worry time” in the early evening. During this time, people are encouraged to write down the thoughts that are causing them to feel anxious. They then write down possible solutions to these worries. Should they wake up in the night, they can then remind themselves that they have attended to these worries, have done all they possibly can, and tomorrow is the next time when they will consider them again.
OTHER METHODS OF CONTROLLING THOUGHTS
Unwanted and intrusive thoughts are believed to be one of the main reasons for a delay in going to sleep (Borkovec, 1982; Espie, 1991). It is therefore important to consider ways of tackling this problem, particularly as patients may make their own efforts to control their thoughts in ways that are ultimately unhelpful. Many patients say that they find it difficult to carry out cognitive restructuring exercises in bed, and indeed it can be argued that any attempt to do so reduces the chances of sleep. Attempts to suppress thoughts can lead to a rebound effect such that the thoughts become more present (Wegner et al, 1987), and it has been suggested that this is an important maintaining factor in anxiety (Salkovskis, 1989) and possibly insomnia (Harvey, 2002b). We suggest that people use imagery distraction techniques or articulatory suppression, a thought-stopping technique, to focus attention away from negative and arousing cognitions when in bed. In the use of imagery, we follow Harvey and Payne’s (2002) suggestion that the person imagine an interesting and engaging situation of his or her own choice that is pleasant and relaxing. The person is asked to avoid imagery that may lead to arousal. To aid the establishment of the image, the person is asked to imagine it in the group and to give a detailed description of it. Articulatory suppression involves the constant repetition of an emotionally neutral, single-syllable word (such as the), at a rate that suppresses other thoughts; the syllable or word needs to be spoken subvocally rather than just imagined, and the person needs to concentrate on saying the word. It was argued by Harvey (2002b) that, theoretically, this technique represents thought suppression and may lead to rebound effects, increasing unwanted thoughts and therefore insomnia. This technique, however, has been reported by Levey and colleagues (1991) as having beneficial effects, and in line with this our own clinical experience is that one third or more of our patients report some benefit from using the technique. Patients also report that they pay less attention to their tinnitus while saying (subvocalizing) the word. Because of the possible counterproductive effects, we are careful to recommend that patients attempt this technique only in combination with a prebedtime session of cognitive restructuring or problem-solving exercises.
Conclusion
Complaints about sleep disturbance are ubiquitous in patients with medical problems and are a key feature in the presentation of tinnitus patients. It has been argued that improving sleep facilitates healing, well-being, and the ability to cope with illness (Shapiro et al, 1993). Improving the sleep of tinnitus patients may not “heal” tinnitus, but the other points in this argument seem as relevant to people with tinnitus as to those with other health problems. Overall, however, clinical effectiveness studies of psychological treatment for tinnitus have not produced encouraging results in the management of insomnia (Andersson and Lyttkens, 1999). Reviewing this area, McKenna (2000) noted that in many outcome studies no measures or only very crude measures of sleep disturbance were included. Even where some measure of sleep disturbance was included, treatments were rarely directed, specifically at insomnia management. As yet there is no published outcome study that targets tinnitus-related insomnia as the central variable, and that includes the sorts of measures that are commonly reported upon in the insomnia literature. This chapter describes the clinical approach employed by the authors in the management of tinnitus-related insomnia. The work is informed as much by the insomnia literature as by the tinnitus literature. Our central proposition is that tinnitus is not a sleep antagonist, but that both tinnitus distress and insomnia are provoked by a process akin to anxiety. As yet our assumptions have not been empirically tested, but our work is being systematically evaluated. It is possible at this stage to report only our most preliminary impressions. To date the vast majority of our patients report some benefit from the group therapy. Most achieve their treatment goals, although such goals vary considerably between individuals and are not restricted simply to increased sleep time.
References
Andersson G, Lyttkens L. A meta-analytic review of psychological treatments for tinnitus. Br J Audiol 1999;33:201–210
Axelsson A, Ringdahl A. Tinnitus: a study of its prevalence and characteristics. Br J Audiol 1989;23:53–62
Beck A. Cognitive Therapy and the Emotional Disorders. New York: Penguin; 1976
Beck A, Steer R. Manual of the Beck Anxiety Inventory. San Antonio, TX: The Psychology Corporation/Harcourt, Brace; 1990
Beck A, Steer R, Brown G. Manual of the Beck Depression Inventory. 2nd ed. San Antonio, TX: The Psychology Corporation/Harcourt, Brace; 1996
Borkovec T. Insomnia. J Consult Clin Psychol 1982;50:880–895
Buysse D, Reynolds C, Monk T, Berman S, Kupfer D. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res 1989;28:193–213
Chambers M, Keller B. Alert insomniacs: are they really sleep deprived? Clin Psychol Rev 1993;13:649–665
Clark D. A cognitive approach to panic. Behav Res Ther 1986;24:461–470
Davies S, McKenna L, Hallam R. Relaxation and cognitive therapy: a controlled trial in chronic tinnitus. Psychol Health 1995;10:129–143
Dement WC, Seidel W, Carskadon MA. Daytime alertness, insomnia and benzodiazepines. Sleep 1982;5:S28–S45
Dement WC, Vaughan C. The Promise of Sleep. New York: Delacorte; 1999
Espie CA. The Psychological Treatment of Insomnia. Chichester, UK: Wiley; 1991
Espie CA, Inglis SJ, Tessier S, Harvey L. The clinical effectiveness of cognitive behaviour therapy for chronic insomnia: implementation and evaluation of a sleep clinic in general medical practice. Behav Res Ther 2001;39:45–60
Folmer R, Griest S. Tinnitus and insomnia. Am J Otolaryngol 2000;21(5):287–293
Fowler D, Garety P, Kuipers E. Cognitive Behaviour Therapy for Psychosis: Theory and Practice. Chichester, UK: Wiley; 1995
Gabriels P. Children with tinnitus. In: Vernon JA, Reich GE, eds. Proceedings of the Fifth International Tinnitus Seminar. Portland, OR: American Tinnitus Association; 1995:270–274
Greenberger D, Padesky CA. Mind Over Mood. New York: Guilford Press; 1995
Hallam RS. Correlates of sleep disturbance in chronic distressing tinnitus. Scand Audiol 1996;25: 263–266
Hallam RS, Rachman S, Hinchcliffe R. Psychological aspects of tinnitus. In: Rachman S, ed. Contributions to Medical Psychology. Vol 3. Oxford: Pergamon Press; 1984:31–53
Harvey AG. A cognitive model of insomnia. Behav Res Ther 2002a;40:869–893
Harvey AG. Trouble in bed: the role of pre-sleep worry and intrusions in the maintenance of insomnia. J Cog Psychother 2002b;16:161–177
Harvey AG, Payne S. The management of unwanted pre-sleep thoughts in insomnia: distraction with imagery versus general distraction. Behav Res Ther 2002;40:267–277
Harvey L, Inglis SJ, Espie CA. Insomniacs’ reported use of CBT components and relationship to long-term clinical outcome. Behav Res Ther 2002;40:75–83
Henry JL, Wilson PH. Cognitive behavioural therapy for tinnitus distress: an experimental evaluation of initial treatment and relapse prevention. In: Hazell J, ed. Proceedings of the Seventh International Tinnitus Seminar. Cambridge: Tinnitus and Hyperacusis Centre; 1999:118–124
Idzikowski C, Shapiro C. Non-psychotropic drugs and sleep. In: Shapiro C, ed. ABC of Sleep Disorders. London: BMJ Publishing; 1993
Jakes S, Hallam R, McKenna L, Hinchcliff R. Group cognitive therapy for medical patients: an application to tinnitus. Cognit Ther Res 1992;16(1):67–82
Jakes S, Hallam RS, Rachman S, Hinchcliff R. The effects of reassurance, relaxation training and distraction on chronic tinnitus sufferers. Behav Res Ther 1986;24:497–507
Kentish RC, Crocker SR, McKenna L. Children’s experience of tinnitus: a preliminary survey of children presenting to a psychology department. Br J Audiol 2000;34:335–340
Levey AB, Aldaz JA, Watts F, Coyle K. Articulatory suppression and the treatment of insomnia. Behav Res Ther 1991;29(1):85–89
McKenna L. Tinnitus and insomnia. In: Tyler RS, ed. Tinnitus Handbook. San Diego: Singular; 2000
Mendleson WB. Insomnia: the patient and the pill. In: Bootzin RR, Kihlstrom JF, Schacter DL, eds. Sleep and Cognition. Washington, DC: American Psychological Association; 1990:139–147
Mendelson W, Garnett D, Linnoila M. Do insomniacs have impaired daytime functioning? Biol Psychiatry 1984;19:1261–1264
Morin C. Insomnia: Psychological Assessment and Management. New York: Guilford Press; 1993
Morin CM, Hauri PJ, Espie CA, Spielman AJ, Buysse DJ, Bootzin RR. Nonpharmacologic treatment of chronic insomnia: an American Academy of Sleep Medicine review. Sleep 1999;22:1134–1156
Morin CM, Savard J, Bliss FC. Cognitive therapy. In: Lichstein KL, Morin CM, eds. Treatment of Late-Life Insomnia. Thousand Oaks, CA: Sage; 2000:207–230
Nicassio PM, Mendlowitz DR, Fussell JJ, Petras L. The phenomenology of the pre-sleep state: the development of the Pre-sleep Arousal Scale. Behav Res Ther 1985;23:263–271
Persons JB, Bertagnolli A. Cognitive-behavioural treatment of multiple problem patients: application to personality disorders. Clin Psychol Psychother 1994;1(5):279–285
Reynolds CF, Kupfer DJ, Hoch CC, Sewitch DE. Sleeping pills for the elderly: are they ever justified? J Clin Psychiatry 1985;46(2):9–12
Salkovskis PM. Cognitive behavioural factors and the persistence of intrusive thoughts in obsessional problems. Behav Res Ther 1989;27:677–682
Sanavio E. Pre-sleep cognitive intrusions and treatment of onset-insomnia. Behav Res Ther 1988;26:451–459
Sateia M, Doghramji K, Haurl P, Morin C. Evaluation of chronic insomnia. Sleep 2000;23:243–308
Schneider-Helmert D. Twenty-four hour sleep-wake function and personality patterns in chronic insomniacs and healthy controls. Sleep 1987;10:452–462
Scott B, Lindberg P, Lennart M, Lyttkens L. Predictors of tinnitus discomfort, adaptation and subjective loudness. Br J Audiol 1990;24:51–62
Scott B, Lindberg P, Lyttkens L, Melin L. Psychological treatment of tinnitus: an experimental group study. Scand Audiol 1985;14:223–230
Seidel W, Ball S, Cohen S, Patterson N, Yost O, Dement W. Daytime alertness in relation to mood, performance and nocturnal sleep in chronic insomniacs and non-complaining sleepers. Sleep 1984;7:230–238
Shapiro C, Dement W. Impact and epidemiology of sleep disorders. In: Shapiro C, ed. The ABC of Sleep Disorders. London: BMJ Publishing; 1993:1604–1607
Shapiro C, Falnigan M. Function of sleep. In: Shapiro C, ed. The ABC of Sleep Disorders. London: BMJ Publishing; 1993:383–385
Shapiro C, Devins GM, Hussain MR. Sleep problem inpatients with chronic illness. In: Shapiro C, ed. The ABC of Sleep Disorders. London: BMJ Publishing; 1993:1532–1535
Spielman AJ, Anderson MW. The clinical interview and treatment planning as a guide to understanding the nature of insomnia: the CCNY Insomnia Interview. In: Chorkroverty S, ed. Sleep Disorders Medicine: Basic Science, Technical Considerations and Clinical Aspects. 2nd ed. Woburn, MA: Butterworth-Heinemann; 1999:385–426
Stepanski E, Zorick F, Roehrs T, Young D, Roth T. Daytime alertness in patients with chronic insomnia compared with asymptomatic control subjects. Sleep 1988;11:54–60
Sugarman J, Stern J, Walsh J. Daytime alertness in subjective and objective insomnia: some preliminary findings. Biol Psychiatry 1985;20:741–750
Sweetow RW. Adjunctive approaches to tinnitus patient management. Hearing J 1989;42:38–43
Wegner DM, Schneider DJ, Carter SR, White TL. Paradoxical effects of thought suppression. J Pers Soc Psychol 1987;53:5–13
White C. Cognitive Behaviour Therapy for Chronic Medical Problems. Chichester, UK: Wiley; 2000
Williams A. Insomnia: Doctor I Can’t Sleep. Rochester, Kent, UK: Amberwood; 1996
Williams C. Overcoming Depression: A Five Areas Approach. London: Arnold; 2001
< div class='tao-gold-member'>



