Fig. 1
Comparison of the robotic axillary thyroidectomy (RAT) and robotic facelift thyroidectomy (RFT) remote access approaches. From Dukews, Terris DJ. Alternative approaches to the thyroid gland. Endocrinal Metab Clin North Am. 2014; 43(2): 459–474. Used with permission
Robotic Axillary Thyroidectomy
RAT Advantages and Disadvantages
As with all remote access techniques, the robotic axillary approach leaves no trace of thyroid surgery on the anterior neck. The incision is well hidden in the axilla, and unlike the other endoscopic remote access procedures it does not result in any anterior chest or breast scarring. These cosmetic attributes have made RAT a popular method of treating surgical thyroid disease in certain Asian markets, where hypertrophic scarring is prominent and the neck is considered a highly sensuous area [16–18]. RAT is associated with increased patient cosmetic satisfaction when compared to open procedures [19, 20]. Some authors have also reported decreased pain after RAT [19], while others have noted that reduced postoperative neck pain was accompanied by increased chest wall pain [20].
There are several disadvantages of the technique. The length of the dissection pocket makes stimulating the recurrent laryngeal nerve difficult with the commercial stimulators currently available. The vector of approach involves dissection across the axilla and anterior chest, regions that may be unfamiliar to most head and neck surgeons. Additionally, as the procedure was imported from Asia to Western practices, it has been noted to be more difficult to obtain adequate operative exposure in patients who are tall or obese [21, 22], and obesity contributes to increased operative time [23]. The procedure is most commonly performed utilizing surgical drains and inpatient observation, requirements that represent a step backwards from many of the advances achieved by the minimally invasive anterior cervical thyroidectomy approaches currently available. Finally, a number of serious complications have been reported using this technique in Western practices [21, 23, 24]. These factors, along with cost and several other considerations, have caused many surgeons in North America to question or altogether abandon this procedure [11–13, 25, 26].
RAT Patient Selection
No uniform selection criteria exist for the RAT [21, 24]. The procedure was first reported in patients with both benign and malignant thyroid conditions, with RAT reserved for patients with nodules ≤5 cm and malignant lesions ≤2 cm [7, 9]. Patients were excluded from consideration if they had prior neck surgery, “severe” Graves’ disease, malignancy with extrathyroidal extension, multiple lateral neck nodal metastases, nodal extracapsular spread, or lesions in the dorsal aspect of the thyroid [9]. Patients with substernal or retropharyngeal extension have also been excluded [23].
While the procedure is primarily utilized for unilateral thyroid surgery, bilateral procedures [7, 9, 21, 22] and both central and lateral neck dissections have been reported with this approach [7, 9, 27]. Candidates for lateral neck dissection have metastatic disease limited to 1 or 2 nodes in a single nodal basin and no evidence of extracapsular spread [27].
RAT Operative Details
The remote access robotic axillary thyroidectomy procedure has been reported in detail [7, 9, 21]. The procedure has undergone some modifications and surgeon-specific refinements since its initial description, and a generalized description of the technique is outlined here. After appropriate positioning, the patient’s arm is extended at the shoulder and a 5–6 cm vertical incision is marked in the anterior axilla. The arm is replaced into its natural position to ensure that the planned incision line will be hidden within the axilla. The arm is then extended again and secured to an armrest. Some authors advocate flexing the elbow to minimize the risk of positional nerve injury [21]. If desired, a 1 cm incision is marked on the patient’s chest 2 cm above the nipple line and 2 cm lateral to midline, though many surgeons now omit this extra working port and introduce all the instruments through the axillary incision, as described below.
The axillary incision is made and continued down to the fascia overlying the pectoralis major muscle. A plane is developed between the subcutaneous tissue and the pectoralis major as dissection is continued medially to the midline and superiorly above the clavicle. The sternocleidomastoid muscle (SCM) is identified and the soft tissue overlying it is elevated from the clavicle and sternal notch superiorly. The space between the sternal and clavicular heads of the SCM is opened and the sternal head is retracted ventrally to expose the strap muscles, taking care to avoid injuring the internal jugular vein or its tributaries. The strap muscles are then elevated off the thyroid gland from the sternal notch to the superior pole and across the midline. The omohyoid may be divided if necessary to improve exposure. A fixed retractor system is employed to maintain the operative pocket (Fig. 2).
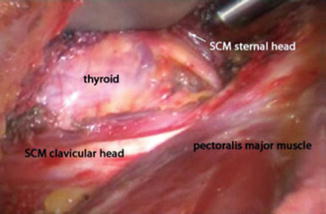
Fig. 2
View of the thyroid between the sternal and clavicular heads of the sternocleidomastoid muscle in the remote access robotic axillary thyroidectomy. From: Lewis CM, Chung WY, Holsinger FC. Feasibility and surgical approach of transaxillary robotic thyroidectomy without CO2 insufflation. Head Neck. 2010;32:121–126. Used with permission
The robot console is then docked on the contralateral side of the operating table. A 30° downward facing camera is utilized. Harmonic shears (Ethicon Endosurgery Inc., Cincinnati, OH) are placed in the dominant arm, and ProGrasp forceps (Intuitive Surgical, Sunnyvale, CA) and a Maryland grasper are placed in the nondominant arms. The camera is inserted through the axillary incision so that the tip is oriented superiorly, while the instruments are inferiorly oriented (Fig. 3).
Fig. 3
Positioning of camera and instrument arms for single incision remote access robotic axillary thyroidectomy. From: Ryu HR, Kang SW, Lee SH, et al. Feasibility and safety of a new robotic thyroidectomy through a gasless, transaxillary single-incision approach. J Am Coll Surg. 2010;211(3):e13–e19. Used with permission
The superior pole is addressed first. The gland is retracted inferiorly, and the superior vascular pedicle is divided with the Harmonic device. The soft tissue attachments and vessels along the inferior aspect of the gland are divided and the gland is rotated medially. The recurrent laryngeal nerve (RLN) and parathyroid glands are identified and preserved. Once these structures have been secured, the isthmus and any remaining soft tissue attachments are divided and the lobe is removed. If a total thyroidectomy is indicated, the superior pedicle of the contralateral lobe is divided, and a subcapsular dissection between the thyroid and the trachea is performed to identify the contralateral RLN and liberate the gland. A surgical drain is placed and the wound is closed in layered fashion. Patients are generally admitted for inpatient observation after the procedure.
RAT Outcomes
RAT has been performed successfully in thousands of patients, mostly in Asia. The mean operative times for RAT vary from 115 to 168 min [7, 9, 28, 29]. Regardless of the approach used or the extent of surgery, remote access robotic thyroid surgery is consistently longer than conventional open thyroid surgery; a review of robotic axillary and bilateral axillo-breast procedures revealed a mean overall increase of 42 min for these approaches when compared to open surgery [20]. However, the overall hospital length of stay is shorter with remote access robotic thyroidectomy than with conventional open surgery [20].
Both central and lateral neck dissections have been described with the RAT approach using combined axillary and anterior chest incisions [9,27,30], with a mean of 6.1 lymph nodes removed from the central neck and 27.7 nodes removed from the lateral neck [27].
The completeness of surgical resection can be reflected in postoperative thyroglobulin (Tg) and 131I uptake levels. Kang et al. [9] reported achieving postoperative Tg levels less than 1 ng/mL in 92 % of patients evaluated, with a mean Tg level of 4.9 ng/mL in the remaining 8 % of patients. A recent systematic review comparing 1,053 RAT patients with 794 open thyroidectomy patients showed no difference in the postoperative Tg levels between these two groups [20]. Kang et al. [30] reported no abnormal 131I uptake levels in 209 patients undergoing total thyroidectomy by RAT followed by postoperative radioactive iodine therapy, though patients undergoing RAT have been reported to have higher postoperative Tg levels than patients having conventional surgery prior to radioactive iodine ablation [29].
RAT subjects patients to all the standard risks of thyroid surgery, and introduces several new ones. Complications such as hemorrhage, brachial plexus neuropathy, chyle leak, Horner’s syndrome, conversion to an open procedure, and tracheoesophageal injury have been reported [9, 21, 23, 28]. Temporary RLN injury has been reported in 0.7–8 % of cases [28, 29], with a permanent RLN injury rate of 0.4 % [28]. Hematoma occurs in up to 2.6 % of cases [29]. Temporary hypocalcemia is seen in up to 41 % of cases [20, 29]. A recent systematic review showed that this risk of transient hypocalcemia was higher in remote access robotic procedures than in conventional thyroidectomy, but there were otherwise no differences in complication rates between the two types of approaches [20].
Robotic Facelift Thyroidectomy
RFT Advantages and Disadvantages
The remote access robotic facelift thyroidectomy offers several distinct advantages over the axillary approach. First, the relevant anatomy and route of dissection are familiar to head and neck surgeons [31]. Second, there is no risk of positional brachial plexus injury, as has been reported with the robotic axillary approach [21, 32]. Finally, the extent of dissection in the RFT approach is less than that of the axillary approach [14]. The shorter distance of dissection facilitates easily stimulation of the RLN, if required, while the reduced volume of dissection permits outpatient recovery without the need for postoperative drains [15].
Despite these advantages, the technique does have some limitations. First, the vector of approach and the robotic instruments currently available do not permit bilateral thyroid surgery through a single unilateral incision. Therefore, the procedure is indicated only in patients for whom unilateral surgery is expected. A completion procedure may be performed through a separate contralateral facelift incision if the final pathology mandates a total thyroidectomy. Second, transient dysfunction of the great auricular nerve is ubiquitous and patients should be counseled to expect temporary numbness of the ear. Third, while it may be technically feasible, no reports of neck dissection using the RFT approach have been published. Therefore this procedure is not recommended for patients who require a neck dissection [15]. Finally, the procedure generally takes longer than does a comparable operation performed via a minimally invasive anterior cervical approach [15, 33].
RFT Patient Selection
Specific patient and disease criteria for RFT have been formalized to maximize the likelihood of operative success and minimize the risk of complications (Table 1) [34]. Patients should be generally healthy and able to tolerate general anesthesia for several hours. Patients should not be morbidly obese, but the presence of a slightly thicker layer of subcutaneous tissue helps protect the integrity of the soft tissue flap. They should have no prior history of neck surgery or radiation. Finally, the ideal patient is highly motivated to avoid a visible cervical scar, understands the limitations and risks of the procedure, and accepts the unlikely but possible chance that conversion to an anterior approach may be required.
Table 1
Indications and contraindications for robotic facelift thyroidectomy
Indications | Contraindications |
|---|---|
– Motivated patient willing to accept increased operative time, increased dissection, and transient ear numbness in exchange for no visible scar – ASA class I or II – No prior neck surgery – Unilateral disease | – Dominant nodule >4 cm – Morbid obesity – Associated lymphadenopathy – Substernal or extrathyroidal extension |
The condition being assessed should also meet certain criteria to be considered appropriate for RFT [34]. Generally, the disease should be amenable to unilateral surgery, such as an enlarging or symptomatic benign nodule or a follicular lesion of undetermined significance. The largest nodule should not exceed 4 cm in its greatest dimension, and there should be no thyroiditis or prior history of thyroid compartment surgery. There should be no substernal component, and no evidence of a high-grade malignancy such as extrathyroidal extension of the lesion or concerning lymphadenopathy.
RFT Operative Details
The remote access robotic facelift thyroidectomy procedure has been described in detail [15, 34]. With the patient sitting upright in the preoperative holding area, a transverse anterior cervical incision is drawn in a natural neck crease in the unlikely event that conversion to an open procedure is necessary. The patient is then positioned just off-center of the operating table toward the side to be operated on. The top of the patient’s head should be almost level with the top of the operating table.
General anesthesia is maintained with a propofol drip, which allows rapid titration of the anesthetic depth. A short-acting muscle relaxant, if necessary, is used to facilitate intubation. The patient is intubated with an EMG endotracheal tube (ETT) to permit intraoperative laryngeal nerve monitoring. A GlideScope (Verathon Inc, Bothell, WA) is useful during intubation so that all members of the operative team can confirm proper positioning of the EMG electrodes. A straight extension is placed on the anesthesia circuit to limit tension on the tubing. A 3-way stop-cock valve connects the CO2 return tubing to the anesthesia circuit to prevent kinking of this tube. The bed is rotated 180° so that the patient’s head is away from the anesthesia provider. The patient’s arms are tucked at their sides and secured with wide silk tape. A formal safety strap that attaches to the table is not used above the patient’s waist because the strap interferes with placement of the retractors. The patient’s head is turned 20°–30° away from the surgical side, with the face supported with soft towels. The anesthesia circuit is taped to the operating table to prevent any excessive tension which might cause the endotracheal tube to twist or migrate.
One centimeter of the occipital hairline is shaved and the facelift incision is marked. The incision begins in the postauricular crease near the inferior extent of the earlobe, and is carried superiorly and then posteriorly into the shaved region of the occipital hairline in a gentle curve that will be obscured by the auricle (Fig. 4). This placement ensures the incision will be completely concealed once the hair regrows. The incision continues posteriorly and inferiorly as far as necessary to ensure adequate exposure.
 < div class='tao-gold-member'>
< div class='tao-gold-member'>




Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
