Thyroid Masses
Vishvesh M. Mehta
Jessica W. Lim
Gady Har-El
Masses of the thyroid gland represent a heterogeneous group of disorders ranging from benign cysts to malignant neoplasms. An estimated 10% to 15% of the U.S. population consult a physician because of a thyroid mass at some point in their life. Each year, approximately 12,000 patients are diagnosed with a thyroid malignancy.
DIFFERENTIAL DIAGNOSIS
Thyroid masses have a diverse differential diagnosis and can be categorized as neoplastic and nonneoplastic (Table 34.1).
Nonneoplastic Masses
Multinodular Goiter
The most common nonneoplastic thyroid mass is multinodular (colloid) goiter (Fig. 34-1). The endemic type of goiter is caused by iodine deficiency, but the sporadic type can occur with adequate iodine dietary levels. Multinodular goiter is more common among women. Nodules vary in size and number. Multinodular goiters can become extremely enlarged, with mediastinal extension and tracheal or esophageal compression (Fig. 34-2). Sudden enlargement may be secondary to hemorrhage within the goiter.
Graves’ Disease
Graves’ disease is an autoimmune disorder that consists of hyperthyroidism, diffuse thyroid enlargement, ophthalmopathy, and myxedema. Progression to hypothyroidism is a late manifestation of this disorder.
TABLE 34-1. Differential diagnosis for thyroid mass | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
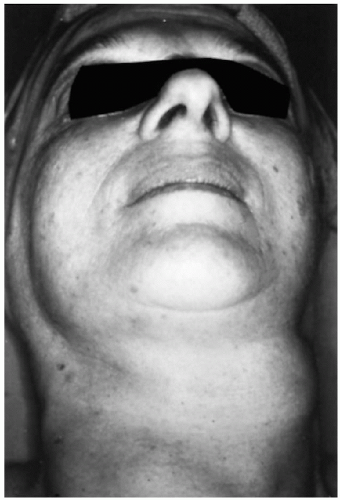 FIG. 34.1. Multinodular goiter of thyroid gland. |
Thyroiditis
Various forms of subacute, granulomatous, or lymphocytic thyroiditis are more common in women. The thyroid gland is generally enlarged and nodular. In subacute thyroiditis, episodic hyperthyroidism may be caused by release of stored thyroid hormone. Tender gland, high erythrocyte sedimentation rate, and increased iodine uptake are the hallmarks of the diagnosis of subacute thyroiditis. Chronic lymphocytic (Hashimoto’s) thyroiditis presents as painless, diffuse nodular enlargement. Patients with this disorder are at increased risk for lymphoma of the thyroid gland. Reidel’s fibrous thyroiditis is a rare, painless process that causes intense induration, making differentiation from neoplasia difficult.
Neoplastic
True neoplasms of the thyroid are classified as benign or malignant. Follicular adenoma is typically a solitary, round, firm, encapsulated lesion of the thyroid gland. Adenomas may undergo cystic degeneration, internal hemorrhage, infarction, calcification, or fibrosis. The nodules usually are hypofunctioning but in rare instances can be hyperfunctioning. Primary malignant neoplasms of the thyroid include well-differentiated (papillary and follicular), anaplastic, and medullary carcinoma as well as lymphoma. The types of malignant neoplasms of the thyroid are listed in Table 34-2.
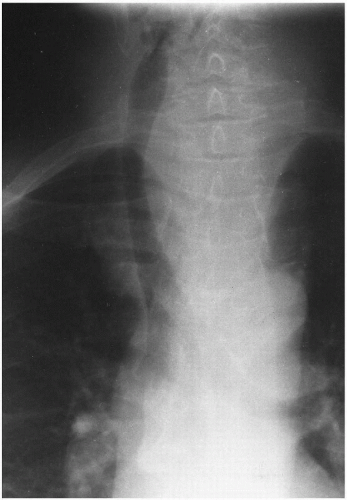 FIG. 34-2. Chest radiograph of patient with thyroid mass shows tracheal deviation caused by mass effect. |
TABLE 34-2. Malignant thyroid neoplasms
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|
|---|