Tonsils and Adenoids
Ramez Habib
Ari J. Goldsmith
The tonsils and adenoids compose Waldeyer’s ring of lymphoid tissue in the human pharynx. Although often grouped together, the tonsils and adenoids are distinct entities. Indeed, the first tonsillectomy was performed in ancient times, but the earliest known adenoidectomy was not performed until the last century. Building on the foundation of this historical context, one must treat the tonsils and adenoids as anatomically unique structures, especially when considering surgical removal. Although removal of these structures constitutes the most commonly performed major surgical procedure in the United States, they remain at the center of controversy as physicians debate indications for surgical removal.
The tonsils and adenoids function as part of the immune system, which explains their location at the portals to the upper aerodigestive tract (Fig. 30-1). Deep crypts with lymphoid follicles in the immediately subepithelial layer provide a large surface area for antigen presentation to an immature immune system. Lymphoid cells mature, recognize these early antigens as self, and therefore do not react to them. In this way, the human upper aerodigestive tract is colonized with a wide variety of indigenous organisms that live everyday in symbiosis. Certain antigens are not recognized as self, and antibodies form in the tonsil and adenoid follicles, leading to the immune response essential for fighting infection.
Several issues regarding adenotonsillar disease often make diagnosis and treatment difficult. Documentation of true tonsillitis or adenoiditis by a trained professional often is lacking when a history of multiple sore throats is obtained from concerned parents. Confirmation of these infections with a positive culture result is even more infrequent and is of questionable necessity. The association between the adenoids and eustachian tubes has only recently begun to be elucidated. The immunologic and developmental roles of the tonsils and adenoids are still not completely appreciated. Furthermore, the immunologic effect of removing these tissues from children or adults is unknown, although most studies have shown improvement in immune function after removal.
The clinical evaluation of children for possible adenotonsillar disease begins with a good history that focuses on the severity of infections and the degree of upper airway obstruction present. The physical examination requires an estimate of tonsil size and degree of obstruction measured on a scale of 1 to 4 (Figs. 30-2 and 30-3). The tonsils are evaluated for the presence of exudate and erythema. The adenoids are more difficult to evaluate, because it can be visualized only with an endoscope or a mirror. It is possible, though, to evaluate the nasal airway for patency, the voice for hyponasality, and the middle ear for the presence of fluid, all of which may be indications of adenoid disease. A high-quality lateral neck radiograph can give a good estimate of adenoid
size and degree of nasopharyngeal obstruction. Adenotonsillar disease and surgical indications can be divided into three main categories: infectious disease, obstructive phenomena, and miscellaneous disease.
size and degree of nasopharyngeal obstruction. Adenotonsillar disease and surgical indications can be divided into three main categories: infectious disease, obstructive phenomena, and miscellaneous disease.
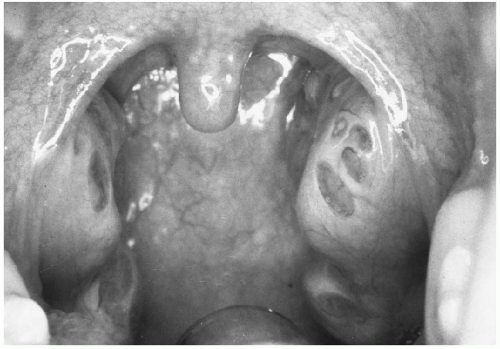 FIG. 30-1. Normal tonsils. |
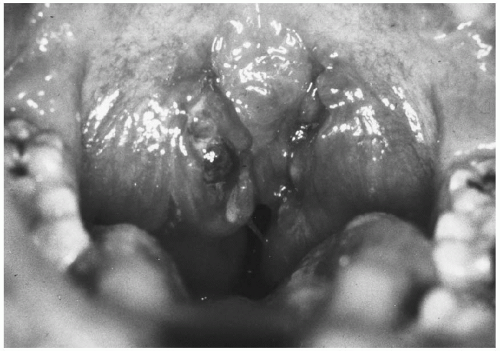 FIG. 30-2. Tonsillar hypertrophy graded 4, or kissing, tonsils.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|