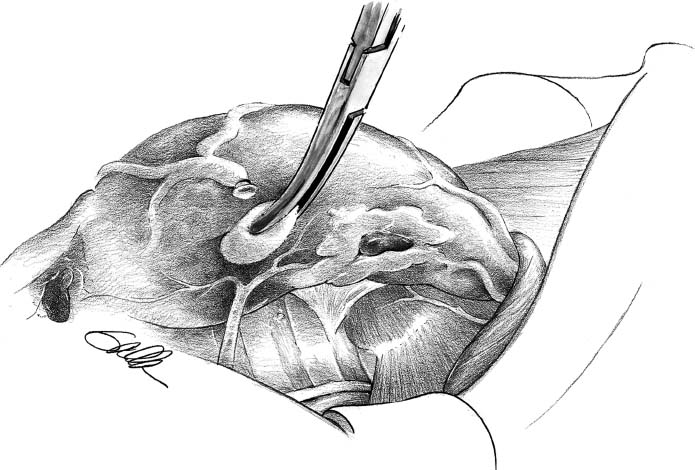
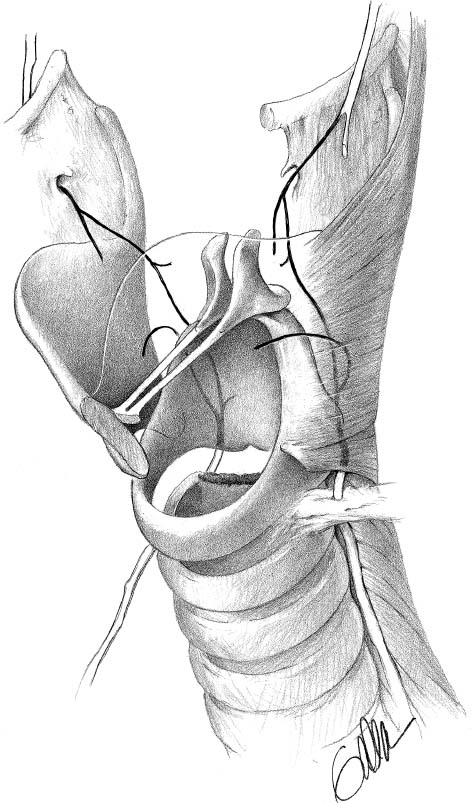
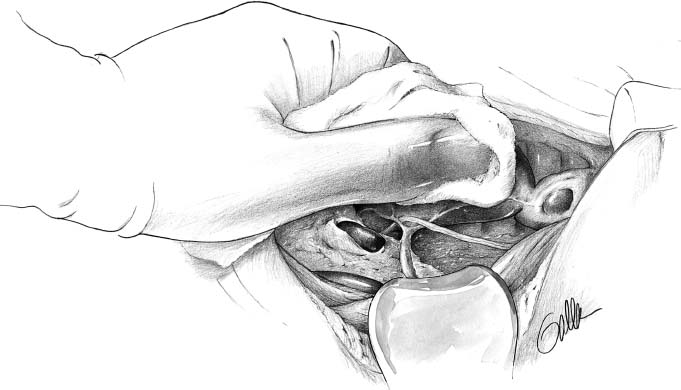
18 The essential point to be made in a discussion of thyroid and parathyroid surgery is that meticulous surgical technique is paramount. This is crucial for appreciation of neck base anatomy, including recurrent laryngeal nerve and parathyroid recognition and preservation. Figure 18–1 The inferior parathyroid can be found adjacent to the inferior pole in thyrothymic horn fat. (From Randolph G. Surgery of the Thyroid and Parathyroid Glands. Philadelphia: Saunders; 2003. Reprinted with permission.) Figure 18–2 The recurrent laryngeal nerve is shown in the tracheoesophageal groove, piercing the ligament of Berry and extending under the inferiormost fibers of the inferior constrictor. The left thyroid cartilage is removed in this illustration to show intralaryngeal nerve anatomy. (From Randolph G. Surgery of the Thyroid and Parathyroid Glands. Philadelphia: Saunders; 2003. Reprinted with permission.) Figure 18–3 The superior parathyroid is identified in fat adjacent to the lateral aspect of the superior pole directly lateral and dorsal to the recurrent laryngeal nerve entry site. (From Randolph G. Surgery of the Thyroid and Parathyroid Glands. Philadelphia: Saunders; 2003. Reprinted with permission.)
Thyroid and Parathyroid Surgery
Gregory W. Randolph
♦ Thyroid Surgery
Surgical Technique
Patient Positioning/Incision
Subplatysmal Skin Flap
Identification of the Airway
Strap Muscles
Inferior Pole
Recurrent Laryngeal Nerve
Superior Parathyroid
Superior Pole
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


