Purpose
To study the tomographic and pathomorphologic features of dome-shaped maculas with swept-source optical coherence tomography (OCT).
Design
Prospective, cross-sectional study.
Methods
The macular area of 51 highly myopic eyes (35 patients) with dome-shaped maculas was studied with swept-source OCT at 1050 nm. Three-dimensional (3-D) data sets were obtained with raster scanning covering a 12 × 8-mm 2 area; 3-D images of the posterior pole were constructed by autosegmentation of the retinal pigment epithelium (RPE).
Results
In all reconstructed 3-D images of the RPE, 2 outward concavities were seen within the posterior staphyloma and a horizontal ridge was formed between these 2 concavities. In 42 of these eyes, this horizontal ridge was band shaped. The vertical OCT section through the fovea showed a convex configuration of RPE, but the horizontal section showed an almost flat RPE line. In 9 eyes, 3-D images showed a typical dome-shaped convexity within the staphyloma. OCT scans showed no outward protrusions in the external scleral surface, but marked scleral thinning was seen consistent with the 2 outward concavities of the RPE. The sclera of the fovea (518.6 ± 97.6 μm) was significantly thicker than that in all 4 quadrants of the parafoveal area (range, 277.2 to 360.3 μm; P < .001).
Conclusions
In highly myopic eyes with a dome-shaped macula, a horizontal ridge is formed within the posterior staphyloma by uneven thinning of the sclera.
High myopia is one of the leading causes of visual disturbance worldwide and is particularly prevalent in Asians. Axial elongation of the globe leads to complex changes in the topography of the posterior pole, with concomitant thinning of the retina, choroid, and sclera and subsequent development of macular pathologic features. Posterior staphyloma, which is one of the characteristic features of high myopia, has been reported to be associated with various vision-threatening complications, including choroidal neovascularization, macular holes, schisis, chorioretinal atrophy, and visual field defects. Using fundus examination, Curtin classified posterior staphyloma in eyes with high myopia into 10 types.
Based on optical coherence tomography (OCT), a dome-shaped macula was first described by Gaucher and associates as an unexpected finding in myopic staphyloma and was characterized as an inward convexity of the macula that occurred in highly myopic eyes within the concavity of a posterior staphyloma. They suggested that the dome-shaped macula may be the result of changes in choroidal thickness or to changes in scleral shape in highly myopic eyes. Subsequently, Imamura and associates, by using enhanced depth imaging OCT, reported that the dome-shaped macula is the result of a localized variation in thickness of the sclera in the macular area. However, the mechanisms that underlie this unusual tomographic feature remain unknown. In addition, most cases of dome-shaped macula in these previous reports were examined by only unidirectional OCT scans. So far, little information is available on the topography of the posterior pole in eyes with a dome-shaped macula.
With the advances in OCT in the last decade, several retinal pathologic characteristics have been identified in highly myopic eyes. However, imaging of highly myopic eyes with conventional OCT systems has several difficulties. Recent OCT generation has used swept-source laser as a light source. The swept-source OCT at a longer wavelength allows deeper tissue penetration into the choroid and even sclera, especially in highly myopic eyes. Additionally, the higher imaging speed, larger scan window, and lower sensitivity roll-off with depth allow for larger scans and the production of 3-dimensional (3-D) images of the posterior pole. In the study described herein, we examined eyes with a dome-shaped macula using swept-source OCT at a longer wavelength to study the pathomorphologic features of the dome-shaped macula by 3-D imaging and to elucidate its association with macular complications.
Methods
The Institutional Review Board and Ethics Committee of Kyoto University approved this prospective study, which adhered to the tenets of the Declaration of Helsinki. Written informed consent for research participation was obtained from each subject before examination.
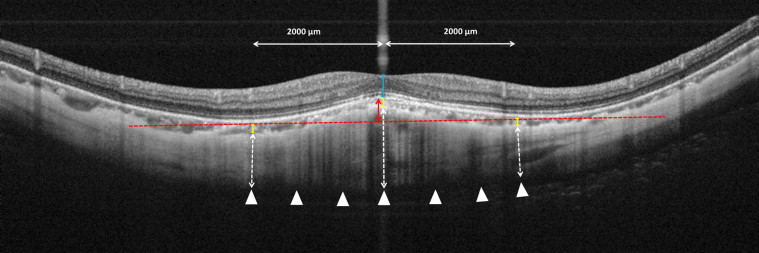
In the current prospective cross-sectional study, we examined 51 eyes (35 patients) with high myopia who demonstrated a dome-shaped macular configuration within the posterior staphyloma. The macular area of the study subjects was examined using a prototype swept-source OCT at Kyoto University Hospital between the beginning of September 2010 and the end of February 2012. The diagnosis of a dome-shaped macula was based on the OCT findings of an inward bulge inside the chorioretinal posterior concavity of the macular area, according to the description of Gaucher and associates. This unusual feature of the macula in eyes with a dome-shaped macula is especially clear on the vertical scans, and performing long vertical scans has been recommended to discern specific features. In the current study, we recruited patients with highly myopic eyes with a dome-shaped macula on the basis of the presence of an inward bulge of the retinal pigment epithelium (RPE) of more than 50 μm on vertical sections of OCT ( Figure 1 ) above a presumed line tangent to the outer surface of RPE at the bottom of the posterior staphyloma. High myopia was defined as a refractive error of −6.0 diopters or more, an axial length of 26.5 mm or more, or both. Eyes were excluded if they had a pre-existing ocular disease or if they had a history of ocular surgery, other than cataract surgery. The original refractive errors were used for eyes that underwent cataract surgery. The type of posterior staphyloma was determined by location and size according to the classification of Curtin. In the current study, eyes with an inferior posterior staphyloma (type V) were excluded. All eyes of our patients had a posterior staphyloma of type I, II, III, or IX.
All subjects underwent a comprehensive ocular examination, including autorefractometry (ARK1; Nidek, Gamagori, Japan), best-corrected visual acuity measurement with a 5-m Landolt chart, axial length measurement using ocular biometry (IOLMaster; Carl Zeiss Meditec, Jena, Germany), slit-lamp examination, intraocular pressure measurement, dilated color fundus photography (TRC50LX; Topcon Corp, Tokyo, Japan), and swept-source OCT examination. All eyes with macular complications underwent simultaneous fluorescein angiography and indocyanine green angiography using Spectralis HRA+OCT (Heidelberg Engineering, Heidelberg, Germany). Eyes with poor images resulting from opaque media (eg, cataracts or corneal opacity) were excluded from the study.
Swept-Source Optical Coherence Tomography and Scan Protocols
The prototype swept-source OCT (Topcon Corp) used in the current study has been described previously. In brief, this swept-source OCT uses a light source of a wavelength-sweeping laser centered at 1050 nm, with a repetition rate of 100 000 Hz. This OCT system has a depth of 2.6 mm in the scan window. Swept-source OCT examinations of the eligible subjects were performed by trained examiners (A.A.E., A.M.) after pupil dilation.
In each subject, multiaveraged horizontal and vertical raster scans of 12 mm were obtained. Fifty single images, where each image consisted of 1024 A-scans, were registered and averaged by software to create a multiaveraged single image. The vertical scan was centered on the fovea, whereas the horizontal scan was centered on the midpoint between the fovea and optic disc.
3-D imaging data sets were acquired by using a raster scan protocol of 512 (horizontal) × 128 (vertical) A-scans per data set in 0.8 seconds. Each raster scan consisted of 128 B-scans and covered an area of 12 × 8 mm 2 centered on the fovea. Centration was confirmed by internal fixation and by a built-in camera within the swept-source OCT system. To improve the signal-to-noise ratio, each image was despeckled by the weighted moving averaging of three consecutive original B-scans. In each image, the RPE line was determined using the built-in automated segmentation-modifying tool, with manual corrections if necessary. 3-D images were constructed to represent the curvature of the posterior pole.
Choroidal and Scleral Thickness Measurement Protocol
Using the multiaveraged OCT images, we measured the choroidal and scleral thicknesses at the center of the fovea and at surrounding parafoveal regions at 2000 μm superiorly, inferiorly, temporally, and nasally, respectively. Retinal thickness was defined as the distance between the vitreoretinal interface and the outer border of the RPE; choroidal thickness was defined as the distance between the outer border of the RPE line and the chorioscleral interface; scleral thickness was defined as the distance between the chorioscleral interface and outer scleral border. Retinal, choroidal, and scleral thicknesses at the fovea were calculated as the average of the measurements in the vertical and horizontal OCT images at the fovea. We also measured the height of the inward bulge of the RPE above a presumed line tangent to the RPE at the bottom of the posterior staphyloma ( Figure 1 ).
The outer surface of the sclera was identified carefully in the OCT scans from retro-ocular structures such as episcleral tissue, the Tenon capsule, inferior oblique aponeurosis, or orbital fat. Scleral tissues were identified by their lamellar morphologic features, continuity of the outer surface of the sclera within the 7 raster lines in the vertical and horizontal scans, and high reflectivity values. The outer border of the sclera at the fovea exceeded the scan window in 2 eyes, and the outer scleral border was not clearly visible in 3 eyes. In these 5 eyes, we used the greatest measurable scleral thickness. In the parafoveal region, the scleral thickness could be identified in all eyes.
Statistical Analysis
Statistical analysis was computed using SPSS statistical software version 16 (SPSS Inc, Chicago, Illinois, USA). All values are expressed as mean ± standard deviation. The measured visual acuity was converted to the logarithm of the minimal angle of resolution (logMAR) units for statistical analysis. The data were analyzed using the unpaired t test. The Fisher exact test was used to analyze categorical variables. Choroidal and scleral thicknesses within different regions were compared using the 1-way analysis of variance with Tukey post hoc analysis. A P value of less than .05 was considered to be statistically significant.
Results
In the current study, 51 eyes of 35 patients (8 men and 27 women) with a dome-shaped macula were studied by swept-source OCT at a 1-μm wavelength. The characteristics of the subjects are summarized in Table 1 . Their mean age was 65.6 ± 11.3 years (range, 40 to 87 years). Mean refractive error was −13.69 ± 5.86 diopters (range, −6.75 to −31.00 diopters), and mean axial length was 29.53 ± 2.16 mm (range, 26.16 to 34.89 mm). Mean visual acuity was 0.36 ± 0.39 logMAR (range, −0.18 to 1.40 logMAR). The dome-shaped macula was bilateral in 16 (45.7%) patients, and all patients were Japanese.
| No. of eyes/patients | 51/35 |
| Sex (male/female) | 8/27 |
| Age (years) | 65.6 ± 11.3 (40 to 87) |
| Axial length (mm) | 29.53 ± 2.16 (26.16 to 34.89) |
| Refractive error (D) | −13.69 ± 5.86 (−6.75 to −31.0) |
| Visual acuity (logMAR) | 0.36 ± 0.39 (−0.18 to 1.40) |
| Intraocular pressure (mm Hg) | 14.8 ± 2.7 (9 to 22) |
| Height of inward bulge a (μm) | 152.3 ± 58.8 (56.0 to 294.0) |
| Foveal retinal thickness (μm) | 190.9 ± 84.9 (0.0 to 522.5) |
| Foveal choroidal thickness (μm) | 34.5 ± 29.0 (10.0 to 117.5) |
| Foveal scleral thickness (μm) | 518.6 ± 97.6 (316.0 to 711.0) |
| Type of posterior staphyloma | |
| I | 18 |
| II | 26 |
| III | 3 |
| IX | 4 |
a The height of the inward bulge was measured from a presumed line tangent to the outer surface of retinal pigment epithelium at the bottom of the posterior staphyloma in the vertical section of optical coherence tomography.
Shape of Inward Protrusion in Eyes With Dome-Shaped Maculas
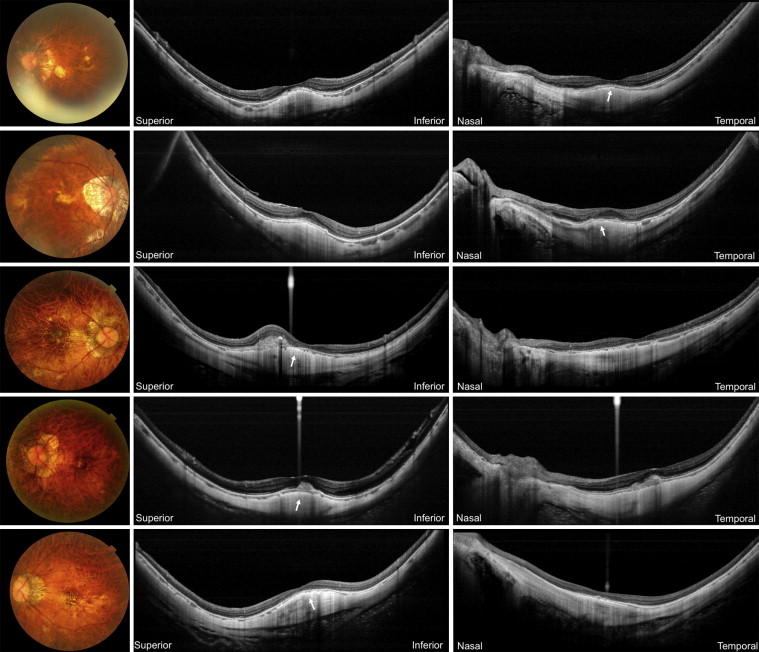
Multiaveraged sections with the swept-source OCT enabled clear visualization of the structure of the retina, choroid, and sclera. In all eyes, an inward bulge within the posterior staphyloma was seen clearly in the vertical sections. The height of the inward bulge above the tangent plane was 152.3 ± 58.8 μm (range, 56.0 to 294.0 μm). In the horizontal scan, however, the inward convexity often was detected less clearly. In some eyes, the horizontal scan showed a flat RPE line without any inward bulge within the staphyloma ( Figure 2 ).
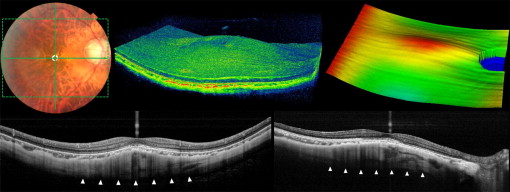
Reconstructed 3-D images revealed curvature of the RPE in the posterior pole. In all eyes, 2 outward concavities of RPE were seen within the posterior staphyloma, and a horizontal ridge was present between these 2 concavities, which was located at the fovea ( Figure 3 , Supplemental Video , and Supplemental Figures 1 and 2 ). In 42 eyes (82.4 %), the horizontal ridge was present as a band shape and the vertical scan through the fovea showed a convex configuration, but the horizontal scan showed an almost flat RPE line. In the other 9 eyes (17.6%), 3-D imaging of the RPE showed a typical dome-shaped convexity within the staphyloma ( Figure 4 ), and both vertical and horizontal OCT scans showed a convex configuration. Of these 9 (17.6%) eyes, the top of the convexity was located beneath the fovea in 7 (13.7%) eyes and was most prominent at the nasal side of the fovea in 2 (3.9%) eyes.

In 2 patients, one eye showed the typical dome-shaped convexity and the other eye showed a band-shaped ridge. There were no significant differences in axial length, refractive error, or choroidal thickness at the fovea or the height of the inward bulge between these 2 types. However, the foveal scleral thickness was significantly thicker in eyes with a dome-shaped convexity (598.3 ± 76.8 μm) than in eyes with a band-shaped ridge (501.5 ± 93.6 μm; P = .006).
Thickness of the Sclera in Dome-Shaped Maculas
Table 2 shows thickness of the choroid and of the sclera in the posterior pole. The choroid showed generalized thinning of the entire posterior pole (34.5 ± 29.0 μm in the fovea). In OCT scans, no outward protrusions were seen in the external surface of the sclera. However, the sclera in the posterior pole showed an uneven thickness consistent with the 2 outward concavities of RPE within the staphyloma. The OCT sections showed marked scleral thinning. In the fovea, the sclera was relatively thick (518.6 ± 97.6 μm) compared with parafoveal areas in all 4 quadrants (range, 277.2 to 360.3 μm; P < .001, respectively). In addition, the scleral thickness was reduced more markedly in the superior and inferior parafoveal areas than in the nasal or temporal parafoveal areas. The scleral thickness at 2000 μm superiorly and inferiorly was significantly less than that nasally ( P < .001 and P = .001, respectively).
| Choroidal Thickness, μm ( P Value a ) | Scleral Thickness, μm ( P Value, a P Value b ) | |
|---|---|---|
| Subfovea | 34.5 ± 29.0 | 518.6 ± 97.6 (NA, < .001) |
| Parafovea at 2000 μm superiorly | 49.8 ± 37.8 (.065) | 277.2 ± 97.1 (< .001, < .001) |
| Parafovea at 2000 μm inferiorly | 40.1 ± 30.4 (.869) | 284.9 ± 91.1 (< .001, .001) |
| Parafovea at 2000 μm temporally | 39.0 ± 29.7 (.940) | 306.0 ± 97.3 (< .001, .040) |
| Parafovea at 2000 μm nasally | 17.8 ± 13.0 (.035) | 360.3 ± 93.5 (< .001, NA) |
a P values, compared with the values in the fovea.
b P values, compared with the values in the nasal area (1-way analysis of variance with Tukey post hoc analysis).
Macular Complications
Table 3 shows the macular complications seen in our patients. Of the 51 eyes with dome-shaped macula, a full-thickness macular hole was seen in only 1 patient (1.9%). Extrafoveal retinal schisis was seen in 9 eyes (17.6%), but foveal schisis was seen in only 1 eye (1.9%). Twenty-one eyes (41.2%) showed choroidal neovascularization (CNV). Of these 21eyes, 12 had been treated with anti-vascular endothelial growth factor agents, 4 had received photodynamic therapy, and 2 had received photodynamic therapy combined with anti-vascular endothelial growth factor agents.
| Choroidal neovascularization | 21 (41.2%) |
| Serous retinal detachment | 3 (5.9%) |
| Diffuse chorioretinal atrophy | 15 (29.4%) |
| Patchy chorioretinal atrophy | 4 (7.8%) |
| Lamellar macular hole | 3 (5.9%) |
| Full-thickness macular hole | 1 (1.9%) |
| Foveal schisis | 1 (1.9%) |
| Extrafoveal retinal schisis | 9 (17.6%) |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


