Purpose
To evaluate the anatomic and functional results of the treatment with intravitreal bevacizumab in complicated retinal arterial macroaneurysm (RAM).
Design
A multicenter interventional, prospective, nonrandomized study.
Methods
Thirty-eight macroaneurysms of 37 patients with foveal complications were evaluated. All patients underwent a comprehensive ophthalmologic examination, fluorescein angiography (FA), and spectral-domain optical coherence tomography (SD OCT) examination. Each patient underwent 3 monthly injections of bevacizumab 1.25 mg/0.05 mL; 3 follow-up visits were planned at week 2, 6, and 12.
Results
Both best-corrected visual acuity (BCVA), expressed in logarithm of minimal angle of resolution (logMAR), and central retinal thickness (CRT) significantly improved during the follow-up visits (0.57 ± 0.21 vs 0.41 ± 0.15 vs 0.23 ± 0.13 vs 0.09 ± 0.10 and 520.38 ± 191.05 vs 396.24 ± 136.18 vs 283.86 ± 71.87 vs 214.84 ± 26.86, respectively, Friedman test P < .0001 for all variables). At 6 weeks of follow-up, FA showed complete closure of the RAM in 36 of 38 cases (94.7%). Four weeks following the third injection, the macular edema had completely resolved and hard exudates regressed slowly in 100% of patients.
Conclusions
Intravitreal bevacizumab is an effective therapy for complicated RAM, quickly improving BCVA and CRT. Anti-vascular endothelial growth factor (VEGF) drugs might actively close the involved pathologically permeabilized retinal artery and normalize the vessel wall formation by localized inhibition of VEGF.
Retinal arterial macroaneurysm is an acquired, localized, fusiform or round dilation of retinal arterial branches that occurs in the posterior fundus. Macroaneurysms predominantly affect older female patients and are often associated with vascular problems such as hypertension or general arteriosclerotic cardiovascular disease. Focal embolic damage to arterial walls is thought to cause retinal macroaneurysms, which result in localized ischemia with vascular endothelial growth factor (VEGF)–induced increased permeability and dilation of the retinal artery.
Although the natural course is usually favorable, some patients with a retinal arterial macroaneurysm may have a sudden loss of vision secondary to abrupt bleeding attributable to rupture of the aneurysm. Hemorrhagic complications often consist of various combinations of subretinal, retinal, sub–internal limiting membrane (ILM), preretinal, and vitreous bleeding. However, even with minimal hemorrhagic complications, some patients experience a gradual visual disturbance attributable to exudation from the aneurysm, which can result in macular edema, serous retinal detachment, and extensive hard exudates in the macular area.
Current treatment options for complicated retinal arterial macroaneurysms rarely lead to improved visual acuity. Observation alone often results in a poor visual outcome in patients with severe macular edema and hard exudates. When macular edema or hard exudates threaten or involve the fovea, prompt diagnosis and early treatment using laser photocoagulation are indicated. Nevertheless, direct laser coagulation of the macroaneurysm has only a limited beneficial effect on visual acuity since severe foveal capillary dropout, as well as scarring after subretinal fluid or hemorrhage, may occur.
Inhibitors of VEGF can prevent the formation of abnormal blood vessels and counteract VEGF-induced vascular permeability. Ranibizumab (Lucentis) has been used in 1 patient with retinal arterial macroaneurysm, with closure of the macroaneurysm leading to resolution of the associated macular edema and, consequently, visual improvement. Bevacizumab (Avastin), an anti-VEGF immunoglobulin G, approved for advanced colon cancer and used off-label in ophthalmology, has been reported to reduce macular edema in 3 patients suffering from ruptured retinal macroanurysm. We present the anatomic and functional results of 3 monthly injections of intravitreal bevacizumab in 37 patients with complicated retinal arterial macroaneurysms.
Methods
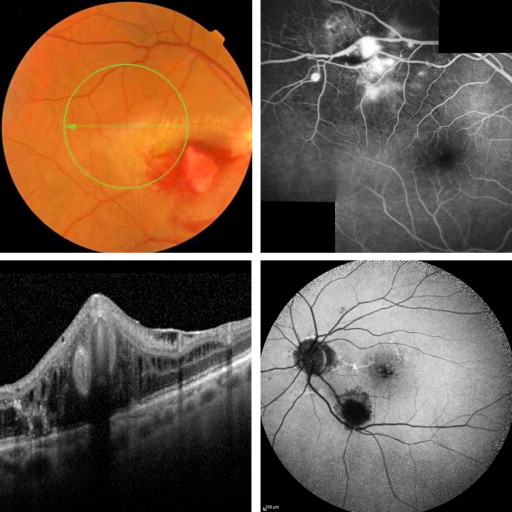
For this clinical study, 41 consecutive patients (41 eyes) with retinal arterial macroaneurysm–associated retinal complications affecting the fovea were evaluated. Patients were examined at Sant’Orsola-Malpighi University Hospital (Bologna), at San Giuseppe University Eye Clinic (Milan), and at Monaldi Hospital (Napoli), between January 2008 and June 2011. The diagnosis of retinal arterial macroaneurysm was based on results of the fundus examination and fluorescein angiography. The angiograms revealed the aneurysm as a pulsating round or ovoid pooling of dye that connected to the retinal artery ( Figure 1 ).
Inclusion criteria included the presence of retinal arterial macroaneurysm in either or both eyes, defined as an acquired dilation of the retinal arteries on biomicroscopy and fluorescein angiography (FA), associated with exudative and/or hemorrhagic manifestations involving the fovea (including subretinal/intraretinal fluid and/or hard exudates and/or hemorrhages) and a best-corrected visual acuity (BCVA) worse than 0.3 logarithm of minimal angle of resolution (logMAR) (20/40 Snellen equivalent). Patients must have been symptomatic for 2 months before considering bevacizumab injections. Eyes with hemorrhagic or exudative changes and other macular abnormalities, such as neovascular maculopathy, retinal vein occlusion, blunt ocular trauma, ocular tumor, or any other condition that could cause hemorrhagic or exudative complications unrelated to retinal arterial macroaneurysm, were excluded from this study.
Patients who met those criteria were enrolled and were regularly scheduled for follow-up at weeks 2, 6, and 12. During each visit, enrolled patients underwent a comprehensive ophthalmologic examination, including refraction and measurement of BCVA, indirect ophthalmoscopy, slit-lamp biomicroscopy, FA, and spectral-domain optical coherence tomography (SD OCT) of the macular region (Spectralis HRA OCT; Heidelberg Engineering, Heidelberg, Germany and Cirrus OCT; Carl Zeiss Meditec, Dublin, California, USA). All SD OCT scans were performed with a scan rate of 40 000 A-scans per second in a 4.5 × 6.0-mm area ( Figure 1 ). Subsequent follow-up scans were carried out at the exact location of the original scan using image alignment software. This image analysis allowed for an accurate determination of quantitative and qualitative retinal changes during follow-up. To verify the accuracy of the SD OCT findings, the fundus area encompassing the lesion was additionally scanned using several vertical and horizontal scans. Retinal thickness of each SD OCT image section was obtained with the volume scan mode. Parafoveal retinal thickness was determined using the retinal thickness of the subfield segments nearest to the retinal arterial macroaneurysm and among the 9 subfields of the Early Treatment of Diabetic Retinopathy Study map, which is composed of 3 rings with radii of 1, 3, and 6 mm, respectively. BCVA measurement was performed by masked staff members who were unaware of the purpose of the study.
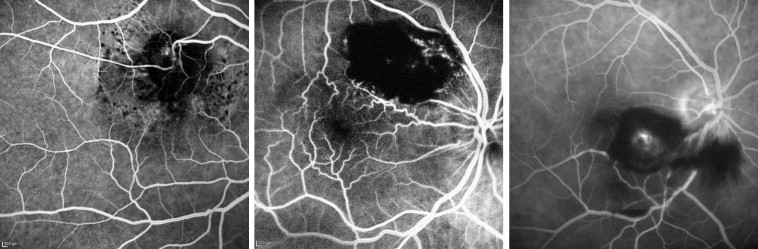
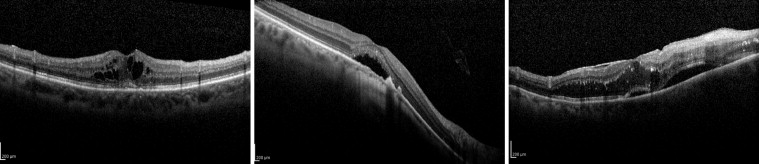
Since the extent of blood-retinal barrier disruption determines the nature of visual impairment, in the present study we classified the retinal arterial macroaneurysms in terms of their barrier function, similar to a protocol first used by Lavin and associates. Hemorrhagic retinal arterial macroaneurysms were defined as retinal arterial macroaneurysms in which hemorrhage is the major component, extending more than 1 disc diameter, and responsible for loss of visual acuity ( Figure 2 ). Exudative retinal arterial macroaneurysms were defined as retinal arterial macroaneurysms in which the exudate is the major component, measuring more than 1 disc diameter and responsible for loss of visual acuity ( Figure 3 ).
After the diagnosis was confirmed, 3 monthly injections of bevacizumab were planned at baseline, week 4, and week 8. The surgical technique consisted of 0.05 mL of intravitreal bevacizumab (Avastin 1.25 mg/0.05 mL; Roche/Genentech, San Francisco, California, USA) injected via a 30-gauge needle under sterile conditions (5% betadine ophthalmic solution), 3.5 or 4.0 mm posterior to the limbus through the pars plana in pseudophakic and phakic eyes, respectively. Postinjection antibiotic prophylaxis was specified as 1 drop of a topical fluoroquinolone 4 times a day for 7 days after injection.
The primary endpoints were reduction of central retinal thickness (CRT) and improvement of BCVA during the follow-up visits. Closure of the retinal arterial macroaneurysm by FA and anatomic resolution of the exudative or hemorrhagic complications, evaluated at week 12, were secondary endpoints. BCVA and CRT differences between patients with hemorrhagic and exudative retinal arterial macroaneurysm presentation were also explored.
All values are presented as mean ± standard deviation (SD). Visual acuity measurements were transformed to logMAR equivalents for statistical analysis. Data were analyzed using the Friedman test for nonparametric repeat measures to evaluate CRT at each of the 4 visits. The Mann-Whitney test was used to compare BCVA and CRT between patients with hemorrhagic and exudative retinal arterial macroaneurysms at each visit. All the statistical analyses were performed using GraphPad InStat version 3.05 for Windows (GraphPad Software, San Diego, California, USA). A P value of <.05 was considered statistically significant.
Results
A total of 37 patients (38 retinal arterial macroaneurysms) were enrolled. We excluded 4 patients with severe hemorrhagic complications, defined as a vitreous hemorrhage that precluded a detailed fundus examination or more than 4 disc areas of hemorrhage. The baseline characteristics of the 37 patients (mean age 76.8 ± 8.2 years, 9 male / 28 female) are reported in Table 1 . A total of 38 retinal arterial macroaneurysms were identified by fluorescein angiography and fundus examination. In all patients, the retinal arterial macroaneurysms were unilateral. One patient had 2 retinal arterial macroaneurysms in the same eye. A history of hypertension was present in 19 of 37 patients (51.3%), ischemic heart disease in 3 of 37 (8.1%), hypercholesterolemia in 8 of 37 (21.6%), aortic aneurysm in 3 of 37 (8.1%), and atrial fibrillation in 4 of 37 (10.8%).
| Patient No. | Age | Sex | No. of RAM | Location | Order of Arterial Tree | Hemorrhagic/Exudative | Past Medical History |
|---|---|---|---|---|---|---|---|
| 1 | 67 | M | 1 | ST | 2 | Exudative | HBP |
| 2 | 83 | F | 1 | ST | 2 | Exudative | |
| 3 | 75 | F | 1 | IT | 2 | Hemorrhagic | HBP,CHOL |
| 4 | 68 | F | 1 | ST | 1 | Hemorrhagic | HBP,IHD |
| 5 | 83 | M | 1 | ST | 3 | Hemorrhagic | |
| 6 | 64 | M | 1 | IN | 1 | Hemorrhagic | HBP |
| 7 | 74 | F | 1 | ST | 2 | Exudative | |
| 8 | 81 | F | 1 | IT | 2 | Hemorrhagic | AF,AAA |
| 9 | 77 | F | 1 | ST | 3 | Hemorrhagic | |
| 10 | 70 | F | 2 | ST | 1 | Exudative | HBP,IHD |
| 11 | 89 | F | 1 | IT | 1 | Hemorrhagic | |
| 12 | 65 | M | 1 | IT | 1 | Exudative | HBP,DVT |
| 13 | 73 | F | 1 | IT | 3 | Exudative | HBP |
| 14 | 88 | F | 1 | IN | 1 | Hemorrhagic | CHOL |
| 15 | 69 | M | 1 | ST | 1 | Hemorrhagic | |
| 16 | 71 | M | 1 | SN | 1 | Hemorrhagic | HBP,DVT |
| 17 | 83 | F | 1 | IT | 1 | Hemorrhagic | |
| 18 | 90 | F | 1 | IT | 3 | Exudative | CHOL |
| 19 | 74 | F | 1 | IT | 2 | Exudative | HBP |
| 20 | 88 | F | 1 | SN | 1 | Exudative | HBP,AF,DVT |
| 21 | 87 | M | 1 | IT | 2 | Exudative | HBP,CHOL |
| 22 | 81 | F | 1 | ST | 2 | Hemorrhagic | HBP |
| 23 | 79 | F | 1 | ST | 1 | Hemorrhagic | HBP,IHD,CHOL |
| 24 | 66 | F | 1 | ST | 1 | Hemorrhagic | |
| 25 | 73 | F | 1 | ST | 1 | Exudative | HBP,AAA |
| 26 | 82 | F | 1 | IT | 3 | Hemorrhagic | |
| 27 | 87 | F | 1 | IT | 2 | Exudative | |
| 28 | 69 | F | 1 | IT | 2 | Exudative | |
| 29 | 78 | M | 1 | IT | 2 | Exudative | CHOL,AF |
| 30 | 70 | F | 1 | ST | 2 | Exudative | |
| 31 | 86 | M | 1 | IN | 1 | Hemorrhagic | HBP,DVT |
| 32 | 73 | F | 1 | IT | 3 | Hemorrhagic | |
| 33 | 69 | F | 1 | IT | 1 | Hemorrhagic | HBP,AF,CHOL |
| 34 | 91 | F | 1 | IT | 1 | Exudative | HBP |
| 35 | 69 | F | 1 | SN | 1 | Hemorrhagic | HBP,CHOL,AAA |
| 36 | 85 | F | 2 | ST | 2,3 | Exudative | HBP |
| 37 | 66 | F | 1 | ST | 1 | Exudative |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


