The Throat
Anatomy and physiology




Oral cavity
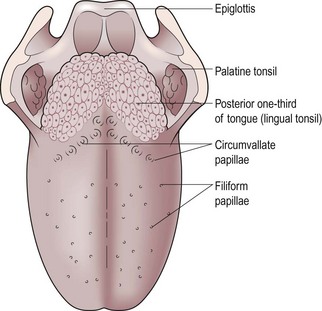
The tongue (Fig. 3.1) is a mass of interlacing muscle contained in a bag of cornified squamous epithelium. It contains numerous taste buds and is essential for efficient articulation, mastication and deglutition.
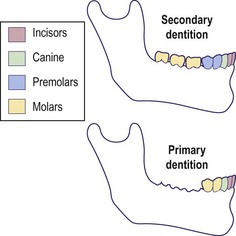
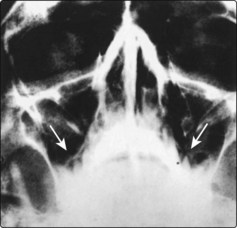
The teeth provide the mechanics for grinding food and are composed of enamel, dentine and cementum. The primary dentition of 20 teeth is completed by about 3 years. There are 32 teeth in the secondary (permanent) dentition commencing at about 6 years and complete by about 18 years (Fig. 3.2). The teeth-bearing alveoli of the maxilla are intimately related to the maxillary sinus. Occasionally the roots of the teeth may rest within the sinus cavity and lead to sinusitis secondary to dental disease.
Pharynx
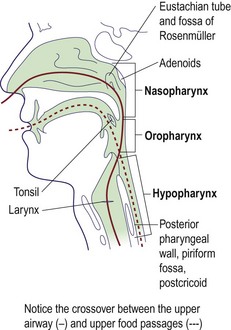
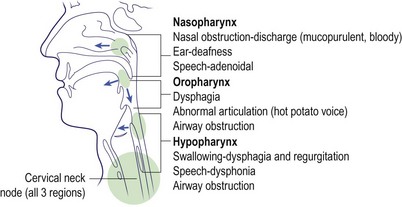
For clinical purposes the pharynx is divided into three regions:



It stretches from the base of the skull above to the cricopharyngeal sphincter below. The oropharynx and hypopharynx, although primarily concerned with swallowing, are so closely related to the laryngeal inlet that pathology in these areas may cause symptoms and signs in adjacent regions. The important clinical structures in each part of the pharynx are shown in Figure 3.3.
Larynx
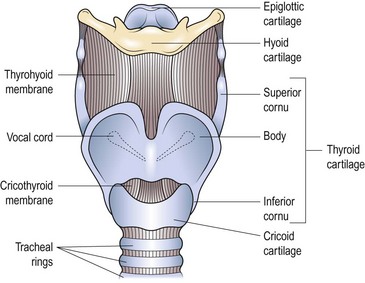
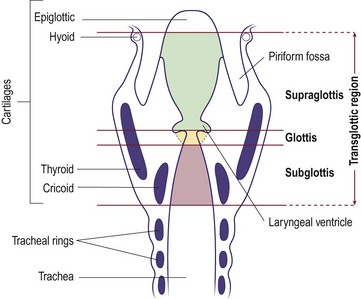
The primary function of the larynx is to protect the tracheobronchial tree. Through evolution it has developed the secondary function of voice production. It has a rigid skeleton consisting of several cartilaginous structures (Fig. 3.4). The most prominent of these is the thyroid cartilage, which inferiorly articulates with the cricoid cartilage. The flap-like epiglottis is attached to the thyroid cartilage and occludes the laryngeal inlet on contraction of the aryepiglottic muscles. The cricothyroid membrane provides a suitable site through which the airway can be maintained in an emergency (see p. 68).
For descriptive purposes the larynx is subdivided into three parts (Fig. 3.5):



Salivary glands
For clinical purposes there are three pairs of salivary glands:



The parotids produce a mainly serous saliva, and the submandibular glands secrete a seromucinous fluid. The parotid duct opens into the buccal sulcus opposite the second upper molar tooth. The submandibular duct opens into the floor of the mouth just lateral to the frenulum of the tongue. The sublingual glands open by multiple small ducts into the submandibular ducts and floor of the mouth. In addition, there are numerous minor salivary glands located throughout the oral cavity and pharynx. The functions of the salivary glands are related to the properties and volume of saliva (Table 3.1).
Table 3.1 Functions of the saliva
Nerve supply
Anatomy and physiology
 Disease in the oropharynx, hypopharynx or larynx may cause problems in adjacent structures.
Disease in the oropharynx, hypopharynx or larynx may cause problems in adjacent structures.
 The functions of the larynx are protection of the lower respiratory tract, phonation and Valsalva.
The functions of the larynx are protection of the lower respiratory tract, phonation and Valsalva.
 Lymph nodes in the neck can become involved in primary and secondary pathologies.
Lymph nodes in the neck can become involved in primary and secondary pathologies.
 An emergency airway can be maintained through the cricothyroid membrane.
An emergency airway can be maintained through the cricothyroid membrane.
Symptoms, signs and examination
Symptoms and signs
Oral cavity
The major signs and symptoms of oral disease include:






Pain
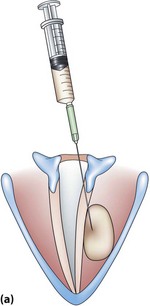
Dental disease is the most common cause of pain in the oral cavity. Carious teeth are tender if subjected to temperature changes and on chewing. Periodontal disease can cause pain on tooth brushing and is associated with halitosis due to accumulation of decaying food debris. Dentures may cause pain if improperly sized, or if they provide an abnormal bite. Atrophy of the teeth-bearing alveolar ridges may result in dentures causing pain, and is commonly seen in the elderly. Maxillary sinusitis may result in toothache if a tooth root is projecting into the sinus mucosa (Fig. 3.6). Pain due to malignant disease is severe and constant, and invariably leads to some degree of dysphagia.
Oral masses
Any complaint of a lump requires palpation of the site, even if a lesion is not visible. Virtually all lumps require biopsy to exclude cancer. Tongue masses are nearly always neoplastic. One exception is the rare, median rhomboid glossitis which presents as a red area on the dorsum of the tongue and is benign (p. 83).
Blockage of a duct of the sublingual salivary gland may give rise to a cystic lesion called a ranula in the floor of the mouth. An exostosis of the hard palate, ‘torus palatinus’, has a typical position in the midline and is hard to palpation (Fig. 3.7).

Pharynx
The precise symptoms are dependent on which region of the pharynx is primarily involved. The majority of pathologies in the oropharynx and hypopharynx, either inflammatory or neoplastic, will lead to some degree of dysphagia (p. 76) (Fig. 3.8). Deafness may occur due to obstruction of the Eustachian tube with nasopharyngeal pathologies. Progressive nasal obstruction and epistaxis with otological symptoms should alert the clinician to nasopharyngeal malignancy. Large oropharyngeal masses may cause a voice change (‘hot potato voice’) and respiratory obstruction.
Examination
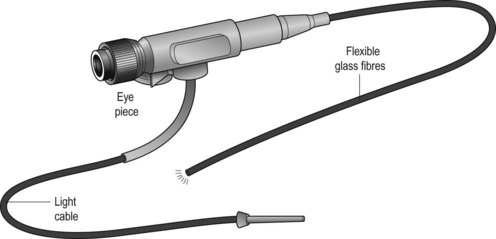
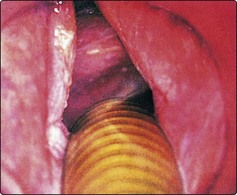
With experience it is possible to view the oral cavity and all parts of the pharynx and larynx using good illumination, tongue depressors and mirrors. These techniques are best learnt under supervision. Increasingly, laryngopharyngeal examination is carried out using a fibreoptic nasal endoscope (Fig. 3.9). Palpation plays a vital role in a full evaluation. Often, a lesion may be more easily felt than visualized, and its limits readily defined. Neck palpation is essential in all cases of head and neck neoplasia.
Imaging
The value of plain radiology of the oral cavity is limited to viewing dental disease. Otherwise, computed tomography (CT) or magnetic resonance imaging (MRI) scanning is superior. However, lateral X-rays of the pharynx are useful, and may show evidence of abnormal shadowing. Contrast swallow studies may provide information on hypopharyngeal and oesophageal pathology (Fig. 3.10). A variety of radiological investigations of the salivary glands are available and are selected according to the suspected pathology (Table 3.2).
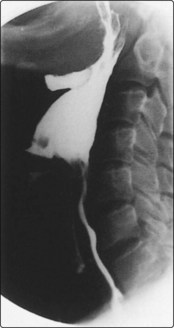
Table 3.2 Imaging techniques available in salivary gland pathology
| Suspected pathology | Imaging mode |
|---|---|
| Submandibular gland calculi | Plain X-ray/ultrasound scan |
| Sialectasis | Sialography |
| Parotid calculi | CT scan/ultrasound scan |
| Neoplasia | MRI/CT |
| Autoimmune disease | Radioisotopes |
Biopsy
Symptoms, signs and examination
 Infective and neoplastic lesions of the upper air and food passages may present as enlarged neck glands.
Infective and neoplastic lesions of the upper air and food passages may present as enlarged neck glands.
 All lumps should be palpated to assess their dimensions, consistency and fixity.
All lumps should be palpated to assess their dimensions, consistency and fixity.
 All parts of the throat can be visualized on an outpatient basis.
All parts of the throat can be visualized on an outpatient basis.
 Contrast studies are required in cases of hypopharyngeal or oesophageal pathology.
Contrast studies are required in cases of hypopharyngeal or oesophageal pathology.
Dysphonia I
Voice changes are often loosely described as hoarseness, but it is preferable to use the terms aphonia and dysphonia. Aphonia should be reserved for cases with no voice or a mere whisper. Dysphonia describes an alteration in the quality of the voice. Laryngeal disorders can present as dysphonia which may progress to stridor (p. 64). Organic causes of dysphonia may be broadly classified as in Table 3.3 and are discussed below. Other causes of dysphonia are considered on pages 62–63.
Table 3.3 Organic causes of dysphonia
| Type | Cause |
|---|---|
| Inflammatory | Acute laryngitis (infective), chronic laryngitis |
| Neoplasia | Carcinoma larynx, respiratory papillomata |
| Neurological | Myasthenia gravis, carcinoma of lung/breast, post-thyroidectomy, spasmodic dysphonia |
| Systemic | Hypothyroidism, rheumatoid arthritis |
Inflammatory laryngeal lesions
Polyps
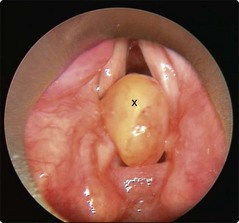
Unilateral inflammatory polyps are not uncommon (Fig. 3.11). The history is similar to acute laryngitis, but resolution of hoarseness cannot occur until the polyp is removed under microlaryngoscopic control. Inhalation of fumes, whether from tobacco, smoke or chemicals, may result in acute dysphonia. All inflammatory lesions, either infection or traumatic, may produce a sufficient degree of oedema to cause respiratory embarrassment.

Chronic laryngitis
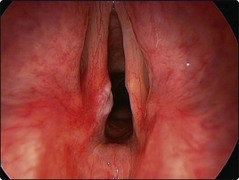
Chronic dysphonia is frequently due to chronic laryngitis. The risk factors are smoking, alcohol, laryngopharyngeal reflux and vocal abuse. The larynx may show hypertrophic epithelium and leukoplakia (Fig. 3.12). Such an appearance may herald neoplastic change, so biopsy is mandatory. If neoplasia has been excluded, management is directed to avoiding known aetiological factors.
Laryngopharyngeal reflux
Gastro-oesophageal reflux disease (GORD) is due to reflux of stomach contents above the lower oesophageal sphincter. Reflux above the lower oesophageal sphincter is called laryngopharyngeal reflux (LPR). The refluxate contains acid, enzymes (pepsin) and bile salts. All of these can be damaging to the larynx. Conventional 24 hour pH studies may not be diagnostic for LPR as they only screen for prolonged reflux episodes with a pH below 4. Transient reflux or less acidic refluxate may not produce heartburn (‘silent reflux’) but still lead to laryngeal symptoms such as dysphonia, cough and throat clearing. LPR is also a risk factor for laryngeal pathology such as chronic inflammation, vocal granulomas and even mucosal metaplasia (Fig. 3.12).
Neurological lesions
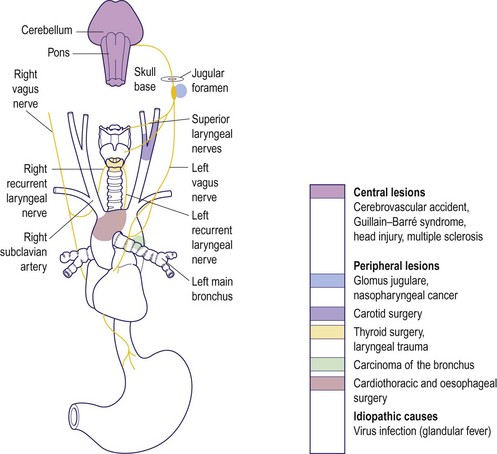
Once a vocal cord palsy has been diagnosed and any local laryngeal pathology excluded, a systematic approach is required to determine the aetiology. This is most easily done by considering the course of the vagus and recurrent laryngeal nerves. Because of its longer route, the left recurrent laryngeal nerve is more frequently involved in pathology (Fig. 3.13). On the left this will be from the cranium via the skull base, neck and thorax back to the larynx; on the right it terminates in the neck. One of the most common causes of vocal cord palsy is malignant disease in the chest or neck, causing recurrent nerve deficits. Inspection of the neck may reveal the scar of previous surgery, e.g. carotid endarterectomy or thyroid surgery (Fig. 3.14). Unilateral vocal cord palsy, where history and examination do not reveal a cause, should therefore have CT imaging from brainstem to chest.

Systemic causes
A number of systemic conditions can produce dysphonia. These include the following:
 Hypothyroidism can produce chronic oedema of the vocal cords. It is improved by appropriate medical therapy.
Hypothyroidism can produce chronic oedema of the vocal cords. It is improved by appropriate medical therapy.


Management
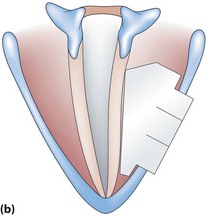
In many cases of unilateral cord palsy, no obvious aetiology is uncovered, despite extensive investigations. Such cases are eventually labelled idiopathic. Some recover spontaneously (which may take up to 6 months) or become asymptomatic as the contralateral mobile vocal cord compensates. If compensation in unilateral cord palsy is inadequate, then a medialization procedure may be beneficial. This involves techniques to medialize the palsied cord so that the mobile cord is more easily able to effect approximation (Fig. 3.15).





Dysphonia II
Dysphonia from non-organic causes may have a psychogenic or habitual aetiology. Specific laryngeal pathology may develop secondary to misuse or abuse of the voice. Table 3.4 classifies non-organic voice disorders. All age groups may be affected.
Table 3.4 Non-organic causes of dysphonias
| Type | Cause |
|---|---|
| Habitual dysphonias | Vocal abuse |
| – acute laryngitis | |
| – vocal nodules | |
| – vocal oedema | |
| – chronic laryngitis | |
| – contact ulcer | |
| Psychogenic dysphonias | Musculoskeletal tension disorders |
| Conversion voice disorders | |
| – muteness | |
| – aphonia | |
| – dysphonia | |
| Mutational falsetto |
Habitual dysphonias
Vocal cord nodules
The nodule is located at the junction of the anterior and middle third of the vocal cord (Fig. 3.16). This is the area of maximum trauma at higher pitch levels seen in activities such as screaming and singing. The dysphonia is breathy and husky with a low pitch quality due to the mass loading of the vocal cords.

Vocal cord oedema and polyps
Mild oedema of the cords may resolve with improvement in the voice. More severe forms, such as Reinke’s, are best treated by microsurgical removal of oedematous tissue, preserving the overlying mucosa (Fig. 3.17). Tissue should always be sent for histological diagnosis.

Contact ulcers
Vocal abuse due to hyperadduction of the vocal folds may result in erosion of surface mucosa; particularly susceptible is the junction of the middle and posterior third of the vocal cord (Fig. 3.18). These are termed contact ulcers and can be sited at the vocal process of the arytenoids. The reaction can sometimes lead to considerable granulation tissue with the formation of a contact granuloma (Fig. 3.19). Gastro-oesophageal reflux may exacerbate or perpetuate this problem.
Psychogenic dysphonia
Musculoskeletal tension disorders
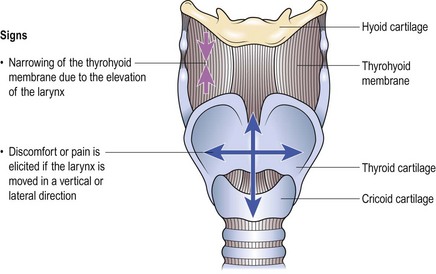
The cardinal features are a dysphonia and the presence of discomfort or pain around the larynx. The clinician can reproduce the pain by palpating the larynx (Fig. 3.21). Occasionally patients may complain of feeling a foreign body in the throat and difficulty in swallowing.
Mutational falsetto (puberphonia)






Stridor
Causes
Stridor results from a wide range of conditions which are summarized in Table 3.5 and discussed below.
Table 3.5 Age-specific causes of stridor
| Age group | Cause |
|---|---|
| Neonatal* | Congenital tumours, cysts |
| Webs | |
| Laryngomalacia | |
| Subglottic stenosis | |
| Vocal cord paralysis | |
| Children* | Laryngotracheobronchitis |
| Supraglottitis (epiglottitis) | |
| Acute laryngitis | |
| Foreign body | |
| Retropharyngeal abscess | |
| Respiratory papillomata | |
| Adults | Laryngeal cancer |
| Laryngeal trauma | |
| Acute laryngitis | |
| Supraglottitis (epiglottitis) |
*Children are at greater risk than adults from upper airway obstruction because their airways are narrower and have softer cartilage, which collapses more easily.
General symptoms and signs of respiratory failure due to airway obstruction are given in Table 3.6.
Table 3.6 Signs of severe respiratory failure due to airway obstruction
Laryngotracheobronchitis


 gross mucosal oedema in the lower respiratory tract
gross mucosal oedema in the lower respiratory tract
 inspiratory stridor, with two-way stridor developing in advanced stages
inspiratory stridor, with two-way stridor developing in advanced stages

Supraglottitis
Supraglottitis (acute epiglottitis) is caused by group B Haemophilus influenzae and is characterized by gross swelling in the supraglottis (Fig. 3.22). It is seen primarily in 3–7-year-olds, although adults may also be affected. Clinical features include:





Subglottic stenosis
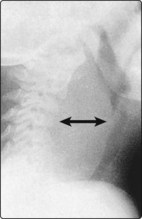
Subglottic stenosis may be congenital. Acquired cases are the result of the trauma of prolonged endotracheal intubation, particularly in premature births (Fig. 3.23). Clinical features include stridor on exertion, or with respiratory infection.

Fig. 3.23 Subglottic stenosis, seen here in a premature birth. The condition can be verified by a neck X-ray.
Foreign body obstruction
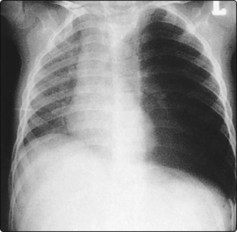
Inhalation of foreign bodies is most common in children. In adults, the problem is usually associated with psychiatric illness or alcohol intoxication. Objects can lodge anywhere in the laryngotracheobronchial tree (Fig. 3.24), and may remain symptomless for long periods. Common symptoms include:
 sudden onset of coughing, wheezing or stridor in a previously healthy child
sudden onset of coughing, wheezing or stridor in a previously healthy child
 chest infection resulting from a foreign body in a smaller airway.
chest infection resulting from a foreign body in a smaller airway.
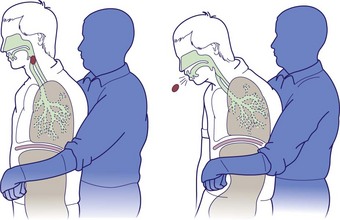
In a child, a foreign body may be dislodged by holding the patient up by the legs and giving a sharp slap on the back. The Heimlich manoeuvre can be used in both adults and children (Fig. 3.25). There should be a low threshold for tracheobronchoscopy in a child who has had a significant choking episode, even in the absence of clinical signs or radiological findings.
Retropharyngeal abscess
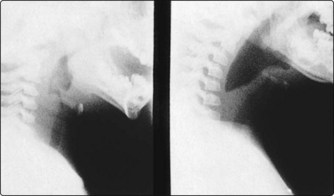
A now rare condition, retropharyngeal abscesses occur mostly in young infants and children. Inflammation and swelling in the retropharyngeal space, secondary to oropharyngeal infection, can cause respiratory embarrassment and severe dysphagia (Fig. 3.26). The child assists breathing by hyperextension of the neck, which is held rigid. Urgent parenteral antibiotics are administered and surgical drainage is performed to avoid spontaneous rupture with risk of inhalation of pus.
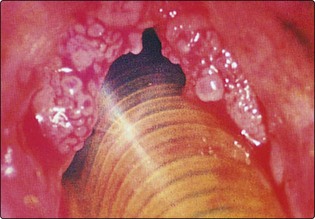
Respiratory papillomata
Respiratory papillomata are characterized by warty lesions appearing in the larynx caused by the human papilloma virus (Fig. 3.27). The trachea, bronchi and pharynx may be involved in florid cases. They are thought to be due to ascending uterine infection; however, acquired cases in adults may be due to genetic predisposition or be sexually acquired. Clinical features include stridor and hoarseness.
Acute laryngitis
Stridor
 Intubation is preferable to tracheostomy in severe cases of laryngotracheobronchitis and supraglottitis.
Intubation is preferable to tracheostomy in severe cases of laryngotracheobronchitis and supraglottitis.
 Suspect an inhaled foreign body in a previously well child who develops abrupt wheezing or stridor.
Suspect an inhaled foreign body in a previously well child who develops abrupt wheezing or stridor.
 Inhaled foreign bodies may remain symptomless for long periods.
Inhaled foreign bodies may remain symptomless for long periods.
 Radiolucent foreign bodies are not uncommon, so do not rely on radiology.
Radiolucent foreign bodies are not uncommon, so do not rely on radiology.

Laryngotracheal injury
The incidence of laryngotracheal trauma has decreased markedly with the compulsory wearing of car seat belts. Most injuries now occur as a result of sporting activities (karate, ice hockey, etc.), but also from knives and bullets. Inhalation of smoke and ingestion of corrosives may cause severe laryngeal oedema. Clumsy laryngeal intubation for anaesthesia, or if required for long-term ventilation, may lead to chronic laryngotracheal problems (Table 3.7).
Table 3.7 Causes of laryngotracheal trauma
| Type | Cause |
|---|---|
| Penetrating injuries | Knives, glass, etc. |



