The role of allergy in chronic otitis media with effusion (OME) is controversial. New evidence from cellular biology and immunology explain the basics of allergic reactions and allow more accurate diagnosis of allergies and inflammatory disease throughout the unified airway. This article examines the epidemiologic, methodological, and immunologic studies of allergic causes of OME, including (1) evidence for and against OME as an allergic disease, (2) allergy as a cause for eustachian tube obstruction, (3) examination of the most sensitive diagnostic tests for allergy, and (4) the effect of treatment of underlying allergies in improving and resolving middle ear disease.
- •
The middle ear, as part of the unified airway, can be a target organ of allergy.
- •
OME is frequently an IgE-mediated, late phase allergic disease.
- •
Allergy can cause eustachian tube dysfunction.
- •
SPT underestimates the incidence of allergy among patients with OME.
- •
Once patients are identified as being atopic, aggressive treatment of their allergies with immunotherapy can frequently resolve the underlying middle ear disease.
Otitis media with effusion (OME) is the major form of chronic relapsing inflammatory disease of the middle ear. It is a clinical disease defined as the presence of fluid in the middle ear behind an intact tympanic membrane with no active infection. For 70 years, the concept of the cause of this disease had been founded on clinical observation. The emergence of molecularly based diagnostic tools in genetics, cell biology, and immunology over the last decade has now enabled us to better understand the pathophysiology of OME and develop new therapies for OME based on the improved understanding.
Chronic OME is associated with hearing loss and delayed speech development and may cause permanent middle ear damage with mucosal changes. It is a disease of immense social and financial impact among families of young children, accounting for more than 16 million office visits a year at an annual cost of more than $3.5 billion (2003) in the United States alone. Children with hearing loss secondary to OME constitute the largest group of people in the world with a reversible learning disorder. Among the 35% of preschool children who experience otitis media (OM), 50% maintain the effusion 14 days after initial treatment. In another study the effusion was found to persist in 70% at 2 weeks, in 40% at 1 month, and in 20% beyond 2 months. Chronic middle ear disease represents an entity with multiple contributing environmental factors interacting with a complex web of immunologic, genetic, mechanical, and inflammatory components.
Many otologists do not embrace a role of allergy in chronic middle ear disease. A recent clinical practice discussion and literature review states that “the relation between allergy and OME will remain controversial until well controlled clinical studies are conducted documenting that in select populations antiallergy therapy is efficacious in preventing or limiting the duration of OME.”
Terminology and definitions
OM describes a symptom, not a disease. It is used to categorize a broad spectrum of middle ear abnormalities, which may involve recurrent acute infections occurring sporadically or extend to conditions of prolonged, ris intact, perforated, or draining.
Chronic suppurative OM (CSOM) refers to a chronic discharge through a perforation of the tympanic membrane. OME is defined by the current gGuidelines as “fluid in the middle ear without signs or symptoms of infection; OME is not to be confused with acute OM (inflammation of the middle ear with signs of infection).” Confusion occurs when practitioners mistakenly equate inflammation with infection.
Allergy refers to symptoms of asthma, rhinitis, or otitis versus atopy, which is a sensitivity as reflected by elevated IgE antibody levels to various allergens without the patient necessarily having the symptoms. There is little research on the role of allergy in OME. Of more than 10,570 articles published from 2001 to 2006 in the 2 major allergy journals ( Allergy and Journal of Allergy and Clinical Immunology ) and the 3 major ear, nose, and throat journals ( Otolaryngology, Head and Neck Surgery ; Laryngoscope ; and Annals of Otolaryngology ), only 16 articles addressed the link of allergy to middle ear disease.
Immunology of allergy
If the nomenclature published by both the European Academy of Allergy and Clinical Immunology and the American Academy of Allergy Asthma and Immunologyguidelines in 2001 and 2003, respectively, for asthma or sinusitis as being either allergic or nonallergic, is extended to categorize inflammation in the middle ear, which is a direct extension of the mucosa-lined respiratory tract, allergic otitis inflammation could be divided into “IgE- or non–IgE-mediated” disease ( Fig. 1 ).
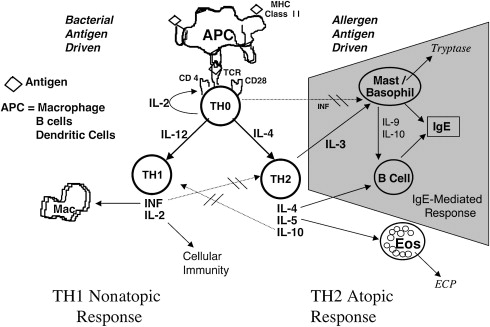
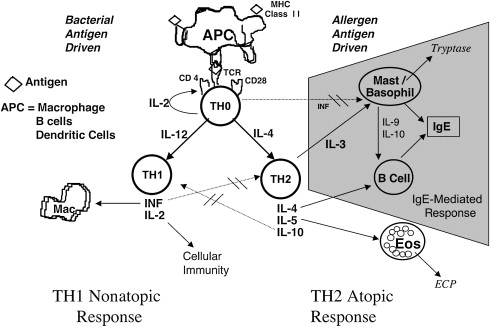
All normal individuals, atopic or not, when exposed during an infection to bacterial antigen stimulate a cell-mediated T H 1 response that is activated by the cytokines interferon γ and interleukin (IL) 2. In the T H 2 allergic reaction, allergens trigger the naive T cell to take a different pathway to become a T H 2 cell ( Fig. 2 ). The immunology of IgE-mediated disease is detailed by Calhoun and Schofieldelsewhere in this issue. Although in summary, IgE-mediated disease is characterized by mast cell degranulation and a classic early phase of symptoms occurring within an hour of antigen exposure, the late phase occurs several hours later and is mediated by the recruitment of eosinophils attracted by IL-5 as well as other cytokines generated during the early phase response. This eosinophil response can be present chronically in ongoing disease. The presence of eosinophils does not in itself implicate IgE-mediated disease but rather reflects non—IgE-mediated hypersensitivity. Influx of eosinophils and their mediators eosinophil cationic protein (ECP) and major basic protein (MBP) are typical of some of the most refractory subtypes of asthma and rhinosinusitis and have been documented in the effusion of OME.
Immunology of allergy
If the nomenclature published by both the European Academy of Allergy and Clinical Immunology and the American Academy of Allergy Asthma and Immunologyguidelines in 2001 and 2003, respectively, for asthma or sinusitis as being either allergic or nonallergic, is extended to categorize inflammation in the middle ear, which is a direct extension of the mucosa-lined respiratory tract, allergic otitis inflammation could be divided into “IgE- or non–IgE-mediated” disease ( Fig. 1 ).
All normal individuals, atopic or not, when exposed during an infection to bacterial antigen stimulate a cell-mediated T H 1 response that is activated by the cytokines interferon γ and interleukin (IL) 2. In the T H 2 allergic reaction, allergens trigger the naive T cell to take a different pathway to become a T H 2 cell ( Fig. 2 ). The immunology of IgE-mediated disease is detailed by Calhoun and Schofieldelsewhere in this issue. Although in summary, IgE-mediated disease is characterized by mast cell degranulation and a classic early phase of symptoms occurring within an hour of antigen exposure, the late phase occurs several hours later and is mediated by the recruitment of eosinophils attracted by IL-5 as well as other cytokines generated during the early phase response. This eosinophil response can be present chronically in ongoing disease. The presence of eosinophils does not in itself implicate IgE-mediated disease but rather reflects non—IgE-mediated hypersensitivity. Influx of eosinophils and their mediators eosinophil cationic protein (ECP) and major basic protein (MBP) are typical of some of the most refractory subtypes of asthma and rhinosinusitis and have been documented in the effusion of OME.
Historical perspective
In 1931, Proetz noted a relationship of middle ear disease with allergic rhinitis. In 1947, Koch observed eosinophilia in the otorrhea from 222 children, “supporting the contention that the middle ear takes part in allergic reactions similar to those seen in the nose and sinuses.” In 1965, Fernandez and McGovern suggested that an allergic mechanism, although not the major cause of chronic OME, was a predisposing factor in as many as 85% of children with acute otitis. Shambaugh suspected allergy as a cause of chronic draining mastoid cavities or middle ears in patients with OME and cautioned that “surgical mastoidectomy, simple or radical is not indicated. With competent allergic diagnosis and management, preferably by the otologist trained in allergic methods, the otorrhea is finally brought under control.”
Objective information on the allergic status of patients with OME is lacking in available otitis databases in Minnesota or Norway (Casselbrant M, personal communication, 2007), making the true incidence of allergy unknown. In studies from 1952 to 1984, Suehs, Senturia and colleagues, Boor, Siirala, Lim and Brick, and Reisman and Bernstein using the techniques of their day, could not find any clinical basis of allergy in the formation of OME. Suehs reported an absence of eosinophils in the middle ear effusion (MEE) of 50 patients, as did Senturia in 1960. Sade and colleagues attributed the basic cause of OME to infection in the nasopharynx with retrograde contamination of the middle ear and edema of the eustachian tube (ET). This thinking has dominated otology to this day.
Allergy testing
Studies that find no increased allergy in subjects with OME often rely on less-objective criteria than actual skin testing to arrive at a diagnosis of allergy. Tomonaga and colleagues criticized many of these methodologically flawed studies in the “Discussion” section of of their work. The study revealed that 21% of 605 patients with allergy had OME, but among 259 patients with OME, 87% were atopic by skin testing, even though only 50% of them had nasal allergy.
The study by Bernstein and colleagues in 1981, although sentinel in being among the first to link allergy to otitis, probably underestimated the role of allergy in OME because it reported that less than 30% of OME was related to allergy. This low percentage results from the very narrow definition of atopy, which required both rhinitis and a total IgE level greater than 100 μg/L or positive results of prick testing. Ten years ago, the author’s group showed that the mean total IgE level among atopic patients was 93.8 μg/L, with two-thirds of atopic patients with OME having a serum IgE level less than 100 μg/L. Otitis is thus similar to rhinitis. It is a “low level IgE disease” having no relation to the total IgE level, unlike asthma, which does show a correlation with IgE levels. Because OME is a low-level IgE disease, prick testing misses more than 80% of patients with OME whose disease actually resolves when those particular allergens that give positive results on intradermal testing are included in their immunotherapy (IT). The reported prevalence of atopy of 81% to 100% by the author among the group of more than 240 patients with OME may reflect the increased sensitivity of intradermal testing compared with results obtained from specific IgE in vitro testing, and/or its equivalent skin prick testing (SPT).
There are several large literature reviews of the relationship of allergy to OME. Ojala surmised that “It would seem that atopy is probably one cause of persistent therapy-resistant otitis media and it must be taken into account when considering the treatment of a chronic ear.” Sprinkle and Veltri found “solid evidence….to suggest that (Gell Coombs) Type I immune injury can be considered a major contributing factor to persistent middle ear effusion.,” and that type III hypersensitivity reactions that require the presence of microorganisms were “very important,” and type IV reactions may also “play a role in causing and potentiating serous otitis media in man.” Doyle concluded that “it has been reasonably well demonstrated that allergy is a risk factor for otitis media.” Skoner and colleagues in his article on OM, with more than 209 references note that “evidence that allergy contributes to the pathogenesis of OME is derived from epidemiologic, mechanistic, and therapeutic lines of investigation.” Tewfik and Mazer concluded “in-vitro and clinical evidence now indicates that, as in asthma and allergic rhinitis, Th2 mediated allergic inflammation is found in middle ear effusion in some patients with OME. As in asthma, this may be a result of direct allergen exposure.”
Epidemiology
OME is a multifactorial disease, of which allergy is only 1 risk factor. Parental smoking, day care classrooms having more than 6 students, asthma, and viral upper respiratory tract infection are also known to predispose one for OME. Yet allergy adds unique comorbidity and is by far a greater risk factor than other identified factors, conferring a 2- to 4.5-fold increased incidence of OME compared with the incidence of OME in nonallergic people. Thus a child who has an episode of acute OM is up to 3 times more likely to develop OME if that same child is also allergic.
Epidemiologic studies in Japan and Sweden have shown a significant relation of allergy to OME. Although only 6% to 20% of the general population is atopic and among atopic patients only 21% have OME, more than 87% of patients with OME were found to be atopic and/or have allergy symptoms. Irander and colleagues found that among 54 Swedish infants, 38% with OME had respiratory tract allergy. Infants with allergic symptoms were 5 times more likely to develop OME than nonatopic patients. Jero and colleagues found similar results in Finland where allergy posed a risk factor of 4.4 for children failing to clear an acute otitis. Allergy certainly puts a patient at risk for recurrent sinus infections because it adds to conditions that can lead to an environment that is suitable for mucostasis, bacterial overgrowth, and chronic inflammation. The author’s group has found that among 97 patients with OME, 62% had documentation of additional atopic signs and symptoms, including asthma in 22%, allergic rhinitis in 48%, eczema in 4%, and chronic nasal congestion in 8%.
Based on SPT, a Greek study found a much higher incidence of allergy among 88 children with chronic OME than in the controls. It was concluded that allergy is an independent risk factor for developing OME. A study in Mexico found that 15% of 80 children with positive skin test result to dust, corn, and cockroach had abnormal tympanograms when compared with 50 controls all of who had normal Type A tympanograms and negative results of SPT for the same 3 allergens. Among children with rhinitis, allergy presented an increased risk for difficulty in opening their ET.
Doner and colleagues evaluated 22 children who required an myringotomy and tubes (M&T) and adenoidectomy. Only 8% of those with no recurrence of their middle ear disease had positive skin test result. This result compared with those of 22 children who had recurrent middle ear effusions requiring repeat M&T. Thirty-eight percent of this group had positive SPT result. The investigators concluded that allergy seemed to be a major contributing factor for recurrent disease.
Viral infections seem to be a trigger for OME. Chonmaitree and colleagues found that 39% of 84 children with MEE had positive viral cultures of their effusion and/or nasal lavage at the time of their acute episode. Only 15% of the patients had no pathogen (bacteria or virus) in the effusion. Other studies showed that human rhinovirus RNA is present in 30% of the effusions of children with OME. Endotoxin has been demonstrated in 52% to 87% of effusions. Polymerase chain reaction has detected the presence of various bacteria in as many as 85% of the cases.
Viral sensitization may contribute to the initial inflammatory process leading to OME. Respiratory syncytial virus (RSV), a common virus in the middle ear and nasopharynx, induces a state of IgE-mediated allergy in the nasopharynx wherein patients with elevated number of mast cells in the adenoid bed are more prone to OME on viral exposure. RSV enhances the synthesis of proinflammatory cytokines (IL-1b, tumor necrosis factor-α, IL-6) and cell adhesion molecules (ICAM-1, ELAM-1, VCAM-1) in the middle ear of infected individuals. Ohashi and colleagues found VCAM-1 levels to be significantly more elevated in the ears of atopic patients. It has been suggested that both a respiratory virus infection and the presence of bacteria in the nasopharynx are required for the development of acute otitis. Garofalo and colleagues examined the effusion from 20 children with acute otitis. They found that tryptase levels were elevated in 79% of the patients. Samples that were negative for viral culture did not contain detectable levels of tryptase. It was suggested that viral pathogens were “an essential trigger or priming factor for mast cell degranulation.” Neither virus nor bacteria alone seems to be capable of causing otitis as frequently as the 2 combined, especially in atopic patients.
Histologic studies
Inflammation is exclusively an in vivo phenomenon that only occurs in living tissues with an active microcirculation. Purulence in the middle ear has previously been shown to elevate levels of both eosinophil and neutrophil mediators. Perpetuation of inflammation, regardless of origin, is the crucial difference between recurrent acute OM and OME. A basic question is whether the middle ear inflammation was the result of infection, allergy, or both. Atopy seems to have a significant relationship to whatever produces a response from eosinophils and mast cells in the middle ear. This is a significant observation not only in regard to the association to allergy but also because human eosinophils are much more toxic than neutrophils, making them particularly harmful to host tissues.
The fact that conventional histology does not readily detect degranulated or activated neutrophils, mast cells, or eosinophils has led to various conclusions and is the major reason this controversy has been perpetuated. There is also disagreement as to whether mediators in MEE come from the plasma or local tissue. In the initial stages of serous otitis, mast cells are found in the lamina propria and the pars flacida of diseased human middle ears. Mast cells release inflammatory mediators producing vasodilatation and mucosal edema, as well as neutrophil chemotaxis. Using animal studies, Nakata and colleagues found few eosinophils in the effusion of immunized chinchillas in the acute phase of inflammation but also concluded that “middle ear effusion is a local product of the middle ear mucosa rather than a transudate from plasma.” Histopathologic examination of effusion demonstrates that eosinophils and neutrophils are integral components in these secretions.
In addition to the cytotoxic effects of ECP, myeloperoxidase (MPO), and tryptase, these mediators are always accompanied by the other proteases, lysozomasol enzymes, and oxidizers that are released simultaneously from their respective cells. ECP attracts other inflammatory cells, including neutrophils, and also delays apoptosis. This may be why the atopic patient continues to produce additional fluid, when compared with the nonatopic patient. This condition was seen in allergic mice, which produced twice the amount of MEE as nonallergic mice on antigen challenge. ECP has also been shown to decrease ciliary function and impair ET clearance.
The very high concentrations of mediators released by eosinophils and mast cells may also account for the great destruction, osteitis, and granulation tissue described on histologic examination of temporal bones from patients with chronic OME. Both heparin and tryptase contribute to fibrosis and bone resorption. This finding may have added significance in understanding the pathophysiology of chronic scarring in the middle ear as well as in the bone destruction observed in cholesteatoma. A prospective study of 117 patients found that “patients with cholesteatoma had a higher prevalence of IgE-mediated hypersensitivity than patients without that condition.” The researchers concluded that “allergy might contribute to chronic otitis media especially in cases with a cholesteatoma.”
One of the unique features of the middle ear response in OME is the involvement of neutrophils. Most atopic patients have increased levels of MPO in addition to ECP in their ear effusion, even though there is no evidence of acute inflammation. Paired samples confirm that in an acutely infected ear, purulent otitis is associated with a significant elevation of both mediators, but with a disproportionately greater elevation of MPO in the infected side when compared with the nonpurulent ear. Yet even in the nonpurulent ear, the levels of MPO were much higher in atopic patients than in nonatopic patients. The inflammatory response to putative inciting agents such as bacterial and viral products may be amplified in atopy, perhaps via IL-8. Another explanation for the increased MPO level reported in nonpurulent MEE is that an increase in neutrophils may occur as a result of weak stimulation of these cells because bacteria are being cleared from the site of inflammation. Bacterial messenger RNA (mRNA) present in otherwise sterile MEE may serve as a stimulus to T-cell activation. Regardless of whether the relationship between allergy and OME is direct or indirect, marked elevation of effusion MPO levels in atopic patients, but very low levels in nonatopic patients, suggests that atopy may contribute to elevated levels of neutrophil activity in OME to a disproportionate degree among atopic patients.
Neutrophils are reported in IgE-mediated late phase reactions in the nose and skin. Thus the presence of neutrophils in MEE is not necessarily an argument against OME being an allergic disease. Atopy contributes to the elevated levels of MPO by causing the atopic child to respond differently to the products of acute inflammation because of its primed inflammatory cells. This is demonstrated most vividly in the classroom struck by a viral upper respiratory tract infection. Whereas most normal children only experience a cold, their atopic classmates frequently go on to trigger asthma attacks requiring nebulizer treatments.
The destructive potential of these mediators in effusion is often overlooked, as is hearing loss, yet serves as a further justification for the removal of this fluid at the time of myringotomy and for prevention of its reoccurrence by appropriate surgical and allergy management. Allergy testing is frequently recommended in children requiring a second set of tubes, in order that this common predisposing factor for OME can be addressed.
ET dysfunction
ET dysfunction (ETD), either extrinsic or intrinsic, is regarded as the underlying pathophysiologic event that leads to most cases of chronic middle ear disease. Causes of ETD include ciliary dysmotility, nasopharynx carcinoma, cleft palate, gastroesophageal reflux, and adenoid hypertrophy, but these causes only account for a minority of patients. Allergy and reflux are the best explanations for the intermittent nature of ETD. Bluestone outlined 4 hypothetical mechanisms by which allergy could be responsible for ETD leading to the production of OME. These mechanisms included (1) the middle ear functioning directly as a shock organ, (2) ETD due to intrinsic mechanical obstruction from inflammatory swelling of the ET itself, (3) inflammatory obstruction of the nose, or (4) aspiration of bacteria-laden allergic secretions from the nasopharynx into the middle ear. As hypothesized, these explanations have all been documented to occur at times because of allergy.
Obstruction of the ET in humans has been clearly demonstrated to result from antigen challenge. The ET has been shown to be involved functionally and morphologically in type I reactions of the nose. In a double-blind protocol, Friedman and colleagues demonstrated that intranasal pollen challenge of atopic individuals produced allergic rhinitis followed by ET obstruction, which did not occur with the placebo. The allergic reaction inhibited even transient dilations of the ET during swallowing. Several other double-blind protocols with intranasal allergen or histamine challenge produced similar severe functional obstruction of the ET. All these results confirm the hypothesis that the ET may become dysfunctional due to allergic inflammation causing intrinsic mucosal edema and obstruction. Skoner and colleagues in their review state, “much of the research into OM pathophysiology has indicated that there is a pivotal role for allergen-induced dysfunction of the Eustachian tube… Allergen-induced blockage subverts the normal mechanism of gas exchange between the middle ear and the environment, thus setting the stage for development of middle ear underpressured OME.”
The most frequently cited objection of past decades to the allergy hypothesis is that an allergen is unlikely to get into the middle ear itself because of the structural gatekeeper function of the ET. Possible mechanisms of immune response in the ear have been proposed. Secretory immunity does not rely on the premise of direct allergen transport to the middle ear, but rather depends on the newer understanding of both humoral and cell-mediated immunology. These concepts are best explained in the section “Unified Airway.”
Evidence-based medicine has dispelled previously held assumptions. It has been shown that “there are no substantial differences in ET function between ears that develop OME recurrence and ears that do not.” It is also a commonly held myth that the ET will grow to normal size as children mature despite evidence that there is no difference in the size of either the isthmus or the pharyngeal portion of the ET in children with OME versus normals. Sade and colleagues showed that the ET of patients with OM does not have an “immature morphology.” Parents are also falsely told that their otitis-prone children cannot equalize the pressure in their middle ears, yet the fact is that there is no organic obstruction or stenosis of the ET in patients with OME. Only 11% of patients with active OME have abnormally high opening pressures. Finally, there is the myth of antibiotics. Rosenfeld and Bluestone have shown that a meta-analysis of all treatment studies demonstrate antibiotics to be no better than placebo in treating chronic OME. Chronic OME is usually not an infection.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


