The Riedel Procedure
William Lawson
INTRODUCTION
Surgery of the frontal sinus has evolved over the past two centuries from external, morbid procedures to minimally invasive endoscopic techniques. Improvements in imaging, endoscopy, and surgical technique have revolutionized the treatment of sinus pathology and set a new standard of care. Of all the paranasal sinuses management of the frontal sinus is often the most challenging and controversial. Surgical navigation has expanded the role of endoscopic frontal sinus surgery but difficult exposure, restenosis, and neo-osteogenesis limit its applicability. External approaches are an essential component of the surgeon’s armamentarium in the treatment of chronic frontal sinusitis, but are generally limited to failed endoscopic management. Trephination, fronto-ethmoidectomy, and osteoplastic obliteration play an integral role for patients who have undergone several failed internal and external procedures for chronic sinusitis. The Riedel procedure is an obliterative, cosmetically disfiguring technique. Although seldom performed, it provides the only definitive treatment for chronic osteomyelitis of the frontal sinus.
The history of surgery of the frontal sinus may be broadly divided into four periods: (1) external ablative and drainage surgery, (2) external ventilatory procedures, (3) external conservative procedures, and (4) internal conservative procedures. The evolution marks the transition from the preantibiotic era when acute and chronic frontal sinusitis carried great morbidity and mortality. The surgical options were external drainage, removal of diseased bone, and attempts to ventilate the sinus by restoration of patency of the outflow tract.
External approaches to the frontal sinus originated in Europe, in the late 19th century. Ogston, in 1884, and Luc, in 1886, described trephination of the anterior table to perform curettage and to establish drainage of the sinus into the nose through the ethmoid cells using tubes. Nebinger, in 1890, modified this method to provide external drainage via the trephine site. Kuhnt, in 1895, reported a radical method performed through a brow incision. He removed the entire anterior wall of the frontal sinus, curetted the contents of the sinus, and removed the floor of the sinus. The resulting deformity, the long period of convalescence needed, and failure to obliterate deep sinuses were the disadvantages of this method. In 1894, Jansen attempted to render this procedure cosmetically appealing by preserving the anterior wall of the sinus. Ritter, in 1906, modified Jansen’s technique by removal of a portion of the anterior wall to gain better access to the recesses of the sinus.
In 1898, Riedel advocated the most radical procedure, in which he removed the anterior wall and floor of the sinus, the frontal process of the maxilla, and the anterior ethmoid cells. Although the Riedel procedure yielded the best cure with obliteration, the resultant cosmetic deformity remained its major drawback. Killian, in 1903, attempted to minimize the deformity by preserving a portion of the supraorbital ridges; however, this was done at the expense of less successful obliteration. He also advocated a time-consuming reconstruction of the nasofrontal duct with a mucosal flap. In 1908, Knapp described the transorbital removal of the floor of the sinus along with an extensive external ethmoidectomy. Acceptable cosmetic results and complete removal of associated ethmoid disease made this a popular procedure. However, the external frontoethmoidectomy (Lynch-Howarth procedure) resulted in many long-term failures mainly due to restenosis of the nasofrontal duct.
In 1912, Lothrop advocated the formation of a large common nasofrontal duct by removal of the frontal sinus septum, the upper nasal septum, and bilateral ethmoidectomies. Despite creation of a very wide drainage port, fibrosis with stenosis again rendered long-term results unacceptable. Mosher, as late as the 1940s, was a proponent of radical removal of the posterior and anterior tables of the frontal sinus, along with the floor, to affect obliterative cranialization of the sinus cavity in cases of frontal osteomyelitis. Cranialization of the frontal sinus by removal of the posterior wall has present-day advocates who cite the improved cosmesis achieved when ablation of the sinus becomes necessary in cases of intracranial complications of sinusitis, tumor removal, or severe trauma.
In 1912, Lothrop advocated the formation of a large common nasofrontal duct by removal of the frontal sinus septum, the upper nasal septum, and bilateral ethmoidectomies. Despite creation of a very wide drainage port, fibrosis with stenosis again rendered long-term results unacceptable. Mosher, as late as the 1940s, was a proponent of radical removal of the posterior and anterior tables of the frontal sinus, along with the floor, to affect obliterative cranialization of the sinus cavity in cases of frontal osteomyelitis. Cranialization of the frontal sinus by removal of the posterior wall has present-day advocates who cite the improved cosmesis achieved when ablation of the sinus becomes necessary in cases of intracranial complications of sinusitis, tumor removal, or severe trauma.
The introduction of antibiotics and progressive technologic improvements in imaging and instrumentation were pivotal in directing sinus surgery to cosmetically acceptable and conservative endoscopic techniques. In this regard, the frontal osteoplastic flap was a watershed procedure. The technique of raising a hinged periosteal (osteoplastic) flap in frontal sinus surgery was described in the 19th century by Kocher, Schonborn, and Brieger in Europe. Beck, MacBeth, and others stressed the utility of radiographic templates to enhance safety of the procedure. Bergara in South America and Montgomery and Goodale in North America were pioneers in developing the frontal osteoplastic flap with adipose tissue obliteration in its modern form. Subsequently, this operation became the most popular external technique for the frontal sinus due to its improved cosmetic results and success rates in eradicating chronic infections of the frontal sinus.
The introduction of fiberoptic endoscopes has rendered the intranasal cannulation and enlargement of nasofrontal outflow tract technically feasible, effective, and with greater safety. Intranasal methods of trephination into the frontal sinus are not new. Rasping, drilling mucosal flaps, stenting, and extensive ethmoidectomies, as well as procedures to destroy or reconstruct the nasofrontal duct endonasally, have been in use since the turn of the 20th century. However, failing to maintain long-term patency of the nasofrontal duct has continued to be a problem with recurrent infection and mucocele formation. Endoscopic modification of the Lothrop procedure in which both nasofrontal ducts are joined together to create a larger common outflow tract with a greater chance of continued patency was introduced by Draf.
Comprehensive reviews of the history of intranasal and external surgical approaches to the frontal sinus exist, and early bibliographical citations can be found in these landmark articles. However, to date, there still remain a small number of cases of refractory chronic frontal sinusitis exhausting the surgical armamentarium of experienced sinus surgeons. These include cases that have failed multiple intranasal and external procedures, including osteoplastic obliterative techniques. Implicit in the continuing failure of medical and surgical management is the development of chronic osteomyelitis, which now must be treated aggressively to stop further spread in the bone and intracranial complications. In this context, a radical ablative procedure becomes mandatory.
HISTORY
The typical patient requiring the Riedel procedure has undergone multiple sinus surgeries. Generally, both endoscopic and open sinus procedures have been performed over a period of many years or even decades, yet the patient continues to have complaints of chronic frontal sinusitis. The final common pathway is that the frontal bone has developed osteomyelitis. Presenting symptoms may include frontal headache and swelling, active drainage through a sinocutaneous fistula, ocular complaints (diplopia, ophthalmoplegia, proptosis) secondary to orbital involvement, or altered mental status from intracranial involvement.
PHYSICAL EXAMINATION
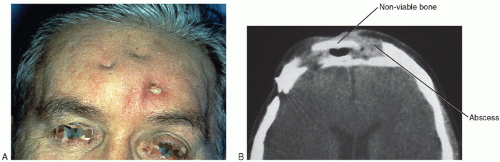
Pathology of the frontal sinus may present with soft tissue, orbital, or neurologic complications. These may become manifest independent of each other or present concomitantly. The most common findings are forehead tenderness, edema, and erythema, consistent with a subperiosteal abscess or Pott’s puffy tumor. Sinocutaneous fistulas and contour deformities occur less often, but represent progression of disease (Fig. 38.1A and B). Orbital complications include diplopia, proptosis, hypoglobus, pre- or postseptal cellulitis, and abscess formation (Fig. 38.2). Formation of epidural or subdural abscesses is a result of infectious spread through the diploë of the posterior table and should be suspected if neurologic signs are present (Fig. 38.3).
INDICATIONS
Chronic osteomyelitis of the frontal bone
CONTRAINDICATIONS
Acute osteomyelitis of the frontal sinus