Purpose
To examine the prevalence of macular telangiectasia type 2 and lesions characterizing it.
Design
Population-based cohort study.
Methods
setting: City and township of Beaver Dam, 1988-1990. study population: A total of 4790 people 43-86 years of age. observation procedure(s): Grading from stereoscopic fundus photographs to measure macular telangiectasia type 2. main outcome measure: Prevalent macular telangiectasia type 2.
Results
Macular telangiectasia type 2 was present at baseline in 0.1% of the population (95% confidence interval [CI] 0.09, 0.1). The frequencies of loss of retinal transparency, crystals in the inner retinal layers, blunted retinal vessels, localized intraretinal pigment migration in the juxtafoveolar region, and presence of yellow deposits and lamellar holes in the foveal area in those without macular telangiectasia type 2 varied from 0.06% for retinal telangiectatic vessels to 1.2% for lamellar holes. Smoking was associated with pigment clumping (odds ratio [OR] per pack year 1.02; 95% CI 1.00, 1.03; P = .02), retinal pigment epithelial (RPE) depigmentation (OR 1.02 per pack year; 95%CI 1.00, 1.04; P = .02), loss of transparency (OR 1.02 per pack year; 95% CI 1.00, 1.03; P = .008), and the presence of a yellow spot in the fovea (OR 2.24 current vs past or never smoker; 95% CI 1.29, 3.89; P = .004), but not with presence of macular telangiectasia type 2 (OR 2.72; 95% CI 0.45, 16.28; P = .27).
Conclusions
The prevalence of macular telangiectasia type 2 (0.1%) is higher than previously thought. These data are useful in estimating the burden of this condition in the population. The role of smoking in the development of macular telangiectasia type 2 requires further study.
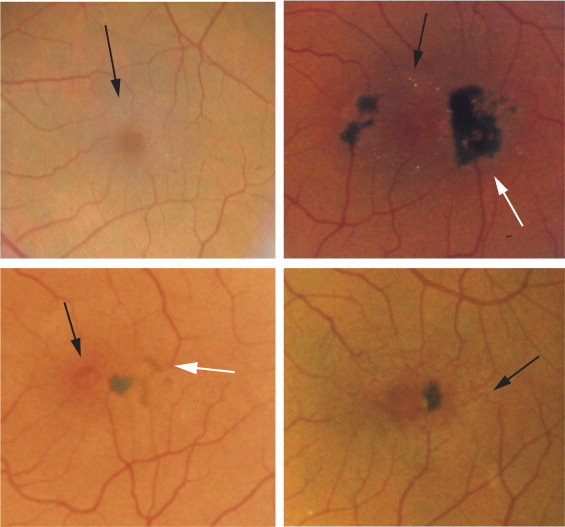
Macular telangiectasia type 2 is characterized by abnormal juxtafoveolar retinal capillaries and is usually accompanied by 1 or more of the following lesions on ophthalmoscopic examination: a loss of retinal transparency, crystals in the inner retinal layers, blunted retinal vessels, and localized intraretinal pigment migration in the juxtafoveolar region and the presence of yellow deposits and lamellar holes in the foveal area ( Figure 1 ). In the earlier stages there is a change in color (gray) and apparent loss of retinal transparency in the juxtafoveolar retina. In its later stages, retinal pigment epithelial (RPE) depigmentation, RPE atrophy, and subretinal new vessels may develop. The pathogenesis of macular telangiectasia type 2 is poorly understood.
Macular telangiectasia type 2 is usually asymptomatic in its earliest stage and is often not discovered until persons, usually in their fifth through eighth decades of life, present with decreased visual acuity. Diagnostically, fluorescein angiography and, more recently, spectral-domain optical coherence tomography (OCT), fundus autofluorescence, and microperimetry testing have been used to identify and characterize macular telangiectasia type 2.
The disease is said to be infrequent. However, there has been only 1 population-based study that described its prevalence using gradings of nonstereoscopic fundus images. The purpose of this paper is to examine the prevalence of macular telangiectasia type 2 and lesions characterizing it in the large population-based Beaver Dam Eye Study.
Methods and Materials
Population
Methods used to identify and describe the population have appeared in previous reports. In brief, a private census of the population of Beaver Dam, Wisconsin, was performed from September 15, 1987, to May 4, 1988, to identify all residents in the city or township of Beaver Dam who were 43 to 84 years of age. Of the 5924 eligible individuals, 4926 participated in the baseline examination between March 1, 1988, and September 14, 1990. Ninety-nine percent of the population was white. Year-5 examinations occurred between 1993 and 1995 in 3722 participants, year-10 in 1998 to 2000 in 2962 participants, and year-15 in 2003 to 2005 in 2375 participants. The fourth follow-up examination began in 2008 and is still in progress. Comparisons between participants and nonparticipants at the time of the baseline and 5-, 10-, and 15-year follow-up examinations have appeared elsewhere.
Procedures and Definitions
Similar procedures, used at both the baseline and follow-up examinations, have been described in detail elsewhere. Pertinent parts of the examination included measuring the refractive error, best-corrected visual acuity for distance, weight, height, and blood pressure, and administering a standardized questionnaire with questions about medications taken and chronic conditions (eg, hypertension, diabetes, emphysema, cardiovascular disease, physical activity). Blood was drawn for measurements of serum lipid levels, white blood cells, platelets, and glycosylated hemoglobin. Stereoscopic 30-degree color fundus photographs centered on the fovea (Diabetic Retinopathy Study [DRS] standard field 1) and the macula (DRS standard field 2) and a single image temporal to the macula (DRS standard field 3) were taken. The presence and severity of lesions associated with macular telangiectasia type 2 ( Figure 1 ) were graded using a standard protocol that evaluates the individual lesions of macular telangiectasia type 2 (loss of retinal transparency, crystalline deposits, dilated tortuous capillaries, blunted retinal vessels, localized intraretinal pigment migration, yellow foveal deposits and lamellar holes in the foveal area, RPE depigmentation, and RPE atrophy) developed prior to beginning grading. Procedures included grading all eyes at baseline for the presence of macular telangiectasia type 2 lesions. Macular lesions consistent with small branch vein occlusion or macular telangiectasia type 1, including lipid exudates, cystoid macular edema, and visible aneurysms, were excluded. If any one of the macular telangiectasia type 2 lesions was graded as questionable or definitely present, a second grading was done by a different grader. If the 2 graders agreed as to the status of the lesions the grading was complete. If the second grader disagreed with the first grader, adjudication was performed by a retinal specialist (R.K.). Additionally, 229 eyes from the same population with no, questionable, or definite macular telangiectasia type 2 lesions were regraded by a different grader at the same time. Twenty-three of these eyes had a lesion regraded from absent to present. Three eyes had a lesion grade changed from present to cannot grade during the adjudication process. The most common lesion changed during the regrade was lamellar hole. All fundus photographs of eyes suspicious for having definite macular telangiectasia type 2 (2 or more different types of macular telangiectasia type 2 lesions) were examined by 3 retinal specialists (B.B., E.C., R.K.). Definite macular telangiectasia type 2 was determined to be present in eyes with 2 or more different types of macular telangiectasia type 2 lesions that were agreed upon by the 3 retinal specialists.
Current age was defined as the age at the time of the examination. Hypertension was defined as a mean systolic blood pressure of > 140 mm H, and/or a mean diastolic blood pressure of > 90 mm Hg, and/or a history of hypertension using antihypertensive medication at the time of the examination. Body mass index was defined as body weight (kg)/height (m 2 ). Cigarette smoking, pack years smoked, and current heavy drinking have been previously defined elsewhere.
Statistical Methods
For these analyses, we examined the prevalence of macular telangiectasia type 2 and the lesions defining it by age and sex. For the purposes of this report, only the 4780 people (97.0%) with at least 1 eye with gradable fundus photographs for macular telangiectasia type 2 without an excluded lesion are included in the analyses. Eyes with epiretinal membranes with traction on the retina or eyes with signs of age-related macular degeneration (AMD) resulting in increased retinal pigment or RPE depigmentation or atrophy were excluded. Also examined were the relationships of risk factors to the prevalence of the lesions. SAS v.9 (SAS Institute, Cary, North Carolina, USA) was used to analyze the data. Multivariate odds ratios (OR) and 95% confidence intervals (CI) were calculated from discrete logistic hazard models (logistic regression for prevalence).
Results
Agreement among graders (absent vs present) for specific macular telangiectasia type 2 lesions varied from 100% (for yellowish spots) to 77% (for lamellar holes). Macular telangiectasia type 2 was present at baseline in 0.1% of the population (95% CI 0.09, 0.1). It was present in 1 woman and 4 men ( Table 1 ). The mean age at baseline of those with macular telangiectasia type 2 was 63.4 (range 52–68) years; the mean age of those without macular telangiectasia type 2 was similar (62.3 [range 43–86] years). None of those with macular telangiectasia type 2 were related. Macular telangiectasia type 2 was bilateral in 2 of the 5 persons. Visual impairment (best-corrected visual acuity of 20/40 or less) was present in 2 affected eyes (29%).
| Baseline VA | Years of Follow-up | Last VA | Lesions Present at Baseline | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Participant | Age | Sex | Eye Involved | Right | Left | Right | Left | Right | Left | |
| 1 | 67 | M | Both | 20/25 | 20/32 | 10 | 20/63 | 20/63 | Blunted retinal vessels | Blunted retinal vessels |
| Loss of retinal transparency | Loss of retinal transparency | |||||||||
| Retinal crystalline deposits | Lamellar hole | |||||||||
| Retinal pigment clumping | Retinal crystalline deposits | |||||||||
| RPE depigmentation | Retinal pigment clumping | |||||||||
| RPE depigmentation | ||||||||||
| 2 | 66 | M | Left | 20/25 | 20/50 | 10 | 20/32 | 20/32 | None | Retinal crystalline deposits |
| Retinal pigment clumping | ||||||||||
| RPE depigmentation | ||||||||||
| 3 | 64 | M | Both | 20/25 | 20/50 | 0 | N/A | N/A | Blunted retinal vessels | Loss of retinal transparency |
| Retinal crystalline deposits | Lamellar hole | |||||||||
| Retinal pigment clumping | Retinal pigment clumping | |||||||||
| RPE depigmentation | Retinal crystalline deposits | |||||||||
| RPE depigmentation | ||||||||||
| 4 a | 52 | M | Left | 20/16 | 20/16 | 20 | 20/32 | 20/25 | Blunted retinal vessels | Blunted retinal vessels |
| Retinal pigment clumping | ||||||||||
| Retinal crystalline deposits | ||||||||||
| RPE depigmentation | ||||||||||
| Retinal telangiectatic vessels | ||||||||||
| 5 | 68 | F | Left | 20/25 | 20/25 | 20 | 20/50 | 20/40 | None | Loss of retinal transparency |
| Retinal pigment clumping | ||||||||||
| Retinal crystalline deposits | ||||||||||
| RPE depigmentation | ||||||||||
a Developed macular telangiectasia type 2 by 10-year follow-up in right eye.
The frequencies of specific macular telangiectasia type 2 lesions in those without macular telangiectasia type 2 were low, varying from 0.06% for retinal telangiectatic vessels to 1.2% for lamellar holes ( Table 2 ). When present, lamellar holes and yellowish spots were more likely to be bilateral ( Table 2 ). Of the 160 eyes with a lesion characterizing macular telangiectasia type 2, 131 (81.9%) had only 1 type of lesion, 26 (16.2%) had 2 types of lesions, 3 (1.9%) had 3 types of lesions, and none had 4 or more types of lesions. When 2 types of lesions characterizing macular telangiectasia type 2 were present, the most common pairs were lamellar holes and yellowish spots in right eyes and blunted vessels and lamellar holes in left eyes. Lesions characterizing macular telangiectasia type 2, when present, were most common in the inner temporal subfield and least frequent in the inner inferior subfield. The presence of any of the lesions in the absence of macular telangiectasia type 2 was unrelated to visual impairment.
| Lesion | # at Risk | # Affected | % Affected | % Bilateral |
|---|---|---|---|---|
| Retinal blunted vessels | 4747 | 56 | 1.18 | 0.00 |
| Retinal pigment clumping | 4738 | 7 | 0.15 | 0.00 |
| Retinal crystalline deposits | 4770 | 10 | 0.21 | 0.00 |
| RPE depigmentation | 4737 | 5 | 0.11 | 0.00 |
| Lamellar hole | 4770 | 56 | 1.17 | 0.02 |
| Retinal telangiectatic vessels | 4759 | 3 | 0.06 | 0.00 |
| Yellowish spot | 4773 | 56 | 1.17 | 0.04 |
| Loss of retinal transparency | 4741 | 10 | 0.21 | 0.00 |
a Estimates in persons without macular telangiectasia type 2. Number at risk varies due to exclusion criteria or inability to grade for a type of lesion.
Smoking was associated with pigment clumping, RPE depigmentation, loss of transparency, and the presence of a yellowish spot in the fovea ( Table 3 ) but not to macular telangiectasia type 2 (OR 2.72; 95% CI 0.45, 16.28; P = .27). Persons with higher hematocrit were less likely and those who were physically active were more likely to have retinal blunted vessels present. White blood cell count was inversely associated with retinal telangiectatic vessels. Platelet count was associated with loss of retinal transparency and inversely associated with macular telangiectasia type 2. Cataract surgery was associated with presence of retinal blunted vessels ( P = .05), retinal telangiectatic vessels ( P = .02), and loss of retinal transparency ( P = .003). No systemic or ocular characteristics were found to be associated with retinal crystalline deposits or lamellar holes. There were no associations of diabetes, hypertension, history of cardiovascular disease, presence of chronic kidney disease, history of aspirin use, or intraocular pressure with any of the lesions characterizing macular telangiectasia type 2 (data not shown).



