Purpose
To report a surgical technique for aqueous misdirection refractory to medical treatment consisting of combined pars plana vitrectomy, hyaloido-zonulectomy, and peripheral iridectomy.
Design
Noncomparative case series.
Methods
The charts of 5 pseudophakic patients who sought treatment for aqueous humor misdirection refractory to medical treatment from May 2008 trough February 2009 were reviewed. All 5 patients underwent anterior vitrectomy, hyaloido-zonulectomy, and peripheral iridectomy with an anterior vitrector through a pars plana incision. Main outcome measures were preoperative and postoperative visual acuity, intraocular pressure, medications, slit-lamp examination results, and fundus findings.
Results
Five female patients (age range, 23 to 89 years) had increased intraocular pressure and shallowing of the anterior chamber after cataract extraction or trabeculectomy, and none responded to conventional medical therapy. After surgery, prompt resolution of the aqueous misdirection was achieved in all cases. The follow-up was 7.6 months (range, 1 to 13 months).
Conclusions
Aqueous misdirection refractory to medical treatment can be treated successfully with surgery consisting of partial pars plana vitrectomy, hyaloido-zonulectomy, and peripheral iridectomy.
Aqueous misdirection, formerly referred to as malignant glaucoma, is a rare condition characterized by elevated intraocular pressure (IOP) and a shallow or flat anterior chamber without pupillary block or choroidal abnormalities. The diagnosis requires the following elements: central and peripheral axial shallowing of the anterior chamber, a patent peripheral iridotomy or clinical slit-lamp examination excluding pupillary block, and the absence of a choroidal effusion or hemorrhage. Aqueous misdirection is unresponsive or aggravated by miotics, but occasionally is improved by cycloplegic therapy, suppression of aqueous humor formation, and hyperosmotics. In this condition, it is thought that aqueous flow is diverted posteriorly into the vitreous cavity. Aqueous misdirection can occur after any type of surgery or spontaneously. It most often occurs after glaucoma surgery, especially in short eyes with a history of angle closure glaucoma, but also can occur after miotic therapy, laser iridotomy, iridoplasty, capsulotomy, cataract extraction, and cyclophotocoagulation. Aqueous misdirection has been described in eyes with no antecedent operation or miotic treatment.
For aqueous misdirection, the following treatments have been described: medical therapy with cycloplegics, aqueous suppressants, and hyperosmotics agents; laser iridotomy and anterior hyaloidotomy (in phakic eyes) or posterior capsulotomy and hyaloidotomy (in pseudophakic eyes); posterior sclerectomy and air injection, with disruption of the anterior hyaloid with a needle at the slit lamp; and complete pars plana vitrectomy. The failure rate of medical and laser therapy is high. We describe herein a technique consisting of pars plana vitrectomy, hyaloido-zonulectomy, and peripheral iridectomy and its results in 5 cases.
Methods
Five consecutive patients with pseudophakic aqueous misdirection who sought treatment for evaluation to the Glaucoma Division of the Jules Stein Eye Institute, University of California at Los Angeles, from May 2008 through February 2009, were included in this study. The diagnosis of aqueous misdirection was established based on the presence of a shallow anterior chamber centrally and peripherally, high intraocular pressure (IOP), exclusion of pupillary block, and the absence of choroidal hemorrhage or effusion.
Medical records of these 5 patients were reviewed and preoperative visual acuity, IOP, slit-lamp examination results, and fundus findings were recorded. All patients underwent a pars plana vitrectomy with peripheral hyaloido-zonulectomy and peripheral iridectomy performed with anterior vitrectomy equipment through a pars plana incision with simultaneous anterior chamber infusion.
Description of Surgical Technique
A paracentesis port was made with a 25-gauge needle, and viscoelastic was injected into the anterior chamber to deepen it slightly. A microvitreoretinal blade then was used to create a clear corneal incision in the anterior chamber. An anterior chamber infusion cannula was placed through this incision and the infusion was turned on while the irrigating solution bottle was placed approximately 30 cm (equivalent to approximately 20 mm Hg) above the patient’s eye.
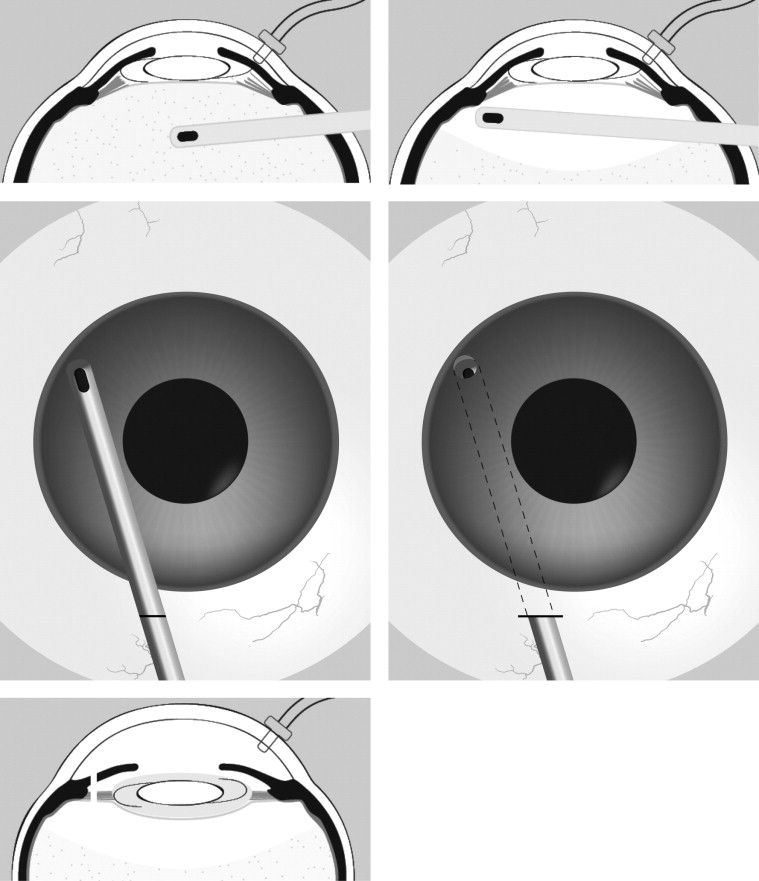
A 5-mm temporal conjunctival peritomy was performed with Wescott scissors and nontoothed forceps. The microvitreoretinal blade was used to make a pars plana incision 3.5 mm posterior to the limbus. The vitrector was inserted through this port behind the intraocular lens ( Figure , Top left). A partial (anterior) vitrectomy then was performed ( Figure , Top right). The length needed for the vitrector to reach the iridotomy site from the sclerotomy was measured outside of the eye and marked ( Figure , Middle left). The vitrector then was turned with the cutter facing up, inserted through the sclerectomy, and used to perform a hyaloidectomy, zonulectomy, and peripheral iridectomy from a posterior approach ( Figure , Middle right). After the creation of this pathway, the anterior chamber depth uniformly deepened immediately ( Figure , Bottom left).
After the vitrector was removed, the scleral incision was closed with a single 9-0 polyglactin suture. Then the infusion was removed and the corneal incision was closed with a single 10-0 nylon suture. The conjunctiva was reattached to the limbus with a 10-0 polyglactin suture.
Results
Patient data are summarized in the Table . The antecedent factors for aqueous misdirection were an uncomplicated phacoemulsification and intraocular lens implantation in 3 cases, trabeculectomy and suture lysis in 1 case, and yttrium–aluminum–garnet (YAG) laser posterior capsulotomy in 1 case. In all 5 cases, the surgery was successful in resolving the aqueous misdirection. The mean follow-up time was 7.6 months (range, 1 to 13 months).
| Case No. | Age (yrs) | Gender | Diagnosis | Previous Surgical Procedures | Visual Acuity | Medications | IOP (mm Hg) | Follow-Up (mos) | |||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Initial | Final | Initial | Final | Initial | Final | ||||||
| 1 | 63 | F | Narrow angle | Phacoemulsification | 20/80 | 20/20 | Atropine, topical hypotensive medication | Topical hypotensive medication | 30 | 14 | 7 |
| 2 | 89 | F | POAG | Phacoemulsification, trabeculectomy + LSL | 20/60 | 20/40 | Atropine, topical hypotensive medication, oral acetazolamide | None | 18 | 8 | 7 |
| 3 | 23 | F | Uveitic glaucoma | Ahmed implant, phacoemulsification, Ahmed revision | CF | 20/40 | Atropine, topical hypotensive medication | None | 18 | 6 | 10 |
| 4 | 47 | F | CACG | Phacoemulsification, YAG capsulotomy | 20/25 | 20/25 | Topical hypotensive medication, oral acetazolamide | Topical hypotensive medication, oral acetazolamide | 26 | 15 | 1 |
| 5 | 48 | F | CACG | Phacoemulsification, Ahmed + YAG capsulotomy | HM | LP | Atropine, topical hypotensive medication, oral acetazolamide | Topical hypotensive medication | 34 | 30 | 13 |
Case 1
A 63-year-old woman had a history of unsuccessfully treated aqueous misdirection in her left eye after cataract extraction. A vitrectomy was performed without significant deepening of the anterior chamber and because of uncontrolled IOP, a Baerveldt valve was implanted in her left eye. She underwent 2 additional vitrectomies in this eye with poor results. The Baerveldt implant was removed and a laser YAG iridotomy was performed. She had a final visual acuity of counting fingers as a result of glaucomatous damage.
She sought treatment for her right eye. She had a nuclear sclerotic cataract and visual acuity of 20/40, with progressive narrowing of the anterior chamber. Cataract surgery was performed in her right eye. After surgery, a shallow anterior chamber and high IOP developed despite medical therapy. On the first day after surgery, her IOP was 31 mm Hg and remained in this range with further shallowing of the anterior chamber. Two weeks after the cataract surgery, a pars plana vitrectomy combined with hyaloido-zonulectomy and peripheral iridectomy was performed. The anterior chamber deepened immediately during surgery and IOP was 20 mm Hg on the first postoperative day. Ten days later, the IOP was 13 mm Hg with timolol administration twice daily. After 7 months of follow-up, visual acuity was 20/20, IOP was 14 mm Hg with topical timolol twice daily in her right eye, and the anterior chamber was deep.
Case 2
An 89-year-old woman with primary open-angle glaucoma sought treatment for glaucoma. She was pseudophakic in both eyes and had a shallow anterior chamber in her left eye. IOP was also higher in the same eye (15 mm Hg in the right eye and 26 mm Hg in the left eye). After failure to control the IOP with maximal medical therapy, a trabeculectomy was performed in her left eye with 3 tight sutures closing a rectangular scleral flap. Four days after trabeculectomy, 1 of the sutures was cut, and 6 days after the suture lysis, the patient had an IOP of 30 mm Hg and a shallow anterior chamber. Treatment with topical steroids twice daily, atropine once daily, and oral acetazolamide 250 mg 4 times a day was initiated. With this treatment, the anterior chamber deepened and the IOP improved, but later recurred with significant central anterior chamber shallowing. At this point, an anterior vitrectomy, hyaloido-zonulectomy, and peripheral iridectomy were performed. The anterior chamber deepened during surgery and the IOP was 11 mm Hg on the first postoperative day. On the third day after surgery, although the anterior chamber was deep, IOP was 6 mm Hg and peripheral choroidals were noted. These resolved in few days. Seven months after the surgery, the visual acuity was 20/40, IOP was 8 mm Hg without medications, and the anterior chamber was deep.
Case 3
A 23-year-old Hispanic female with uveitic glaucoma had Ahmed glaucoma valve implants in both eyes. Two months after surgery, a shallow anterior chamber and high IOP developed in her right eye. Her visual acuity was counting fingers in her right eye and 20/30 in her left eye. IOPs were 8 and 10 mm Hg in the right eye and left eyes, respectively, and a very shallow anterior chamber was present in the right eye. She had undergone phacoemulsification and intraocular lens implantation in her right eye 3 months earlier. A revision of her Ahmed glaucoma valve and an anterior chamber reformation were performed, but the anterior chamber became shallow again and topical atropine was started. However, the IOP slowly increased to 26 mm Hg with further anterior chamber shallowing. An anterior vitrectomy, hyaloido-zonulectomy, and peripheral iridectomy were performed. The anterior chamber deepened during surgery and the IOP decreased to 14 mm Hg on the first postoperative day. There has been no recurrence of the aqueous misdirection. Three months later, the patient underwent a membranectomy of a dense anterior membrane on the intraocular lens. Since then, and after 10 months of follow-up, the anterior chamber has remained deep, visual acuity has improved to 20/40, and IOP is 6 mm Hg without medical therapy.
Case 4
A 47-year-old female with bilateral chronic angle-closure glaucoma had a shallow anterior chamber and high IOP in her left eye. Her right eye was nanophthalmic. She had undergone strabismus surgery during childhood, cataract surgery in both eyes, YAG capsulotomy in her left eye, and selective laser trabeculoplasty in both eyes. She had been diagnosed with aqueous misdirection in her left eye and had been treated with oral acetazolamide and maximal topical hypotensive medical therapy for 3 years. When she sought treatment from us, her IOP was 22 mm Hg and the anterior chamber in her left eye was shallow. She was taking acetazolamide 500 mg twice daily and topical travoprost once daily in her left eye. Visual acuity was 20/400 in her right eye and 20/25 in her left eye. Slit-lamp examination showed a posterior chamber lens in both eyes and a patent peripheral iridotomy in the left eye. Gonioscopy revealed an angle grading of D20s according to the Spaeth classification (a deep iris insertion into the ciliary body face, a 20-degree angle between the iris root and a tangential line to the trabecular meshwork, and a steep iris configuration peripherally, with a few scattered peripheral anterior synechia). On funduscopic examination, there was greater cupping of her left optic nerve with diffuse thinning of the neural rim.
The patient underwent a pars plana vitrectomy, hyaloido-zonulectomy, and peripheral iridectomy in her left eye. After surgery, she had a fully deep anterior chamber, but the IOP was high during the early postoperative phase: 58 mm Hg on the first day, decreasing to 20 mm Hg in the second week after surgery. Four weeks after surgery, the visual acuity was 20/25 in her left eye, the anterior chamber was deep, and her IOP was 15 mm Hg with oral acetazolamide 500 mg twice daily, topical prednisolone twice daily, and bimatoprost once daily in her left eye.
Case 5
A 48-year-old Asian woman with secondary angle-closure glaucoma after retinal detachment in her left eye sought treatment. She had a visual acuity of 20/25 in the right eye and 20/400 in the left eye. She was taking topical brimonidine once daily, latanoprost once daily, and prednisolone twice daily in her left eye. She was pseudophakic in her left eye. IOP was 12 mm Hg in the right eye and 36 mm Hg in the left eye. Gonioscopy showed a D30s angle (a deep iris insertion into the ciliary body face, 30-degree angle between the iris root and a tangential line to the trabecular meshwork, and steep iris configuration according to the Spaeth classification) on the right and a 360-degree closed angle on the left. An Ahmed glaucoma valve implant was inserted in the left eye, and on the first postoperative day, the IOP was 9 mm Hg and the visual acuity was counting fingers. There was a small clot in the anterior chamber. The tube was patent and the anterior chamber was deep. On postoperative day 4, the patient had light perception visual acuity and increased blood in the anterior chamber. A B-scan ultrasound was performed that revealed a large choroidal effusion. The choroidal effusion completely resolved with conservative therapy after 10 days, and successive IOP measurements ranged between 7 and 12 mm Hg. Four months after the tube implant, the patient had significant posterior capsule opacification and a visual acuity of 20/200. A YAG capsulotomy was performed. Eight months later, the patient had a very shallow anterior chamber and an IOP of 24 mm Hg in the left eye. The patient was started on oral acetazolamide 250 mg 3 times daily and topical atropine 1% twice daily, timolol 0.5% twice daily, and brimonidine twice daily, but the IOP increased to 34 mm Hg and there was no deepening of the anterior chamber. At this point, a pars plana anterior vitrectomy, hyaloido-zonulectomy, and peripheral iridectomy were performed. On postoperative day 1, the patient had a deep anterior chamber and an IOP of 5 mm Hg. Ten months later, the patient had some shallowing of the anterior chamber, an IOP of 20 mm Hg, hyphema, and suprachoroidal hemorrhage verified with B-scan ultrasonography. Atropine 1% once daily, timolol 0.5% twice daily, brimonidine twice daily, and prednisolone 3 times daily were started, the anterior chamber deepened, and the IOP decreased to 7 mm Hg. The transient anterior chamber shallowing was attributed to the choroidal hemorrhage. After 13 months of follow-up, the anterior chamber remained deep and the IOP was 30 mm Hg with timolol 0.5% and prednisolone twice daily.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


