CHAPTER 49 The management of eyelid tumors
Having a comprehensive knowledge of the epidemiology, the clinical features of benign and malignant eyelid tumors, an understanding of the relevant tumor biology, and available diagnostic and therapeutic options is essential for the clinician caring for these patients to be able to deliver an appropriate standard of care1.
Epidemiology
Skin cancer is the most common human malignancy with a corresponding human morbidity, mortality, and health care cost. A variety of benign and malignant primary skin, adnexal and other tumors may involve the eyelids, as well as a range of secondary malignancies2. The four relatively common malignant tumors to involve the eyelids are basal cell carcinoma (BCC), squamous cell carcinoma (SCC), sebaceous carcinoma (SC), and malignant melanoma (MM). Additionally almost any other adnexal process can involve the eyelids but these tumors have a very low incidence.
BCC represents about 80% of eyelid malignancies, SCC about 15%, with SC, MM, and other rarer lesions making up the remainder. The age-standardized incidence of BCC ranges from 53 (Germany) to 1041 (Australia) per 100 000 per year3. The age-standardized incidence of SCC is lower, ranging from 11 (Germany) to 499 (Australia) per 100 000 per year. MM incidence in the United States was 24.6 per 100 000 in 20064–6. The Australian incidence is higher; statistics from an Australian cancer registry show an age-standardized incidence rate of 64.4/100 000/year and a mortality rate of 7.1/100 000/year for MM7. The reported incidence in a United States population of SC in whites is 0.11–0.2/100 000/year8, 0.1 in Asian/Pacific Islanders and 0.05/100 000 in blacks9. The incidence in Asians has been reported as much higher, representing 30–40% of all eyelid malignancies in Chinese, Indian, Thai, and Japanese populations10.
The incidence of Merkel cell carcinoma ranges from 0.17 to 0.44/100 000/year in a number of incidence reports, occurring predominately in elderly white males in the head and neck region11–13.
BCC is usually associated with long-term sun exposure14.
Australian studies, where there is a high baseline incidence of BCC, have not shown a strong occupational association, whereas German studies, with a lower baseline incidence, have shown an association with occupational exposure3,15,16. Higher dietary fat intake is associated with a higher incidence of SCC but not BCC17. A population-based study into the association of antioxidant levels and non-melanoma skin cancer (NMSC) incidence, looking at carotenoids, α-tocopherol, and selenium, showed no association with carotenoids or α-tocopherol, but an inverse association between serum selenium levels and the incidence of BCC and SCC18.
Clinical features, diagnosis, and differential diagnosis
BCC typically presents in the fifth to eighth decade of life, most commonly as a well-circumscribed nodular lesion with pearly edges and some telangiectasia, with or without ulceration (Fig. 49.1). These lesions are relatively easy to diagnose clinically but there are many clinical variants which can confound the clinician. Superficial, multifocal BCC may present as flat erythematous plaques; micronodular lesions as multiple small nodules, while the infiltrating, morpheic lesions may have very subtle features and indistinct margins, which make, diagnosis difficult and margins impossible to assess clinically (Fig. 49.2). Less commonly, BCCs may have cystic or pigmented components19.


SCCs may arise de novo, or from a pre-existing actinic keratosis (AK) or areas of squamous intraepidermal carcinoma (IEC, Bowen’s disease, SCC in situ), with appearances that range from erythematous plaques to raised nodular lesions that may be ulcerated, keratotic, or papillomatous (Fig. 49.3)20–22.

Melanomas are generally variably darkly pigmented, but may be amelanotic. They are usually categorized into lentigo maligna melanoma (Fig. 49.4A), superficial spreading melanoma (Fig. 49.8A), nodular melanoma, and acral melanoma. Most melanomas undergo a radial then a vertical growth phase (to be discussed later), such that they present as fairly large flat pigmented macules. The nodular form has a very short or absent radial growth phase and more commonly presents as a dark or reddish-brown nodule. Signs of ulceration clinically usually indicate progression into the vertical growth phase23.




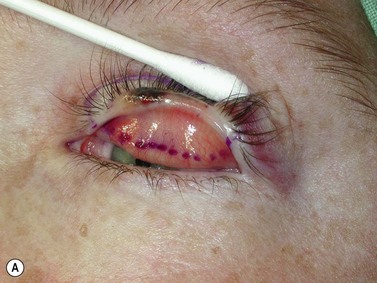




Sebaceous carcinoma is notoriously difficult to diagnose clinically. The lesion may present as a nodule, or as an area of thickening of the tarsal plate associated with a yellow discoloration and ulceration (Fig. 49.5)24–26. Merkel cell carcinoma is also difficult to diagnose clinically, although they usually have a slightly violaceous, purplish hue and grow rapidly.

Probably more important than being able to diagnose each individual lesion correctly at every presentation is the ability to decide whether the lesion is benign or malignant. Further, various clinical features will suggest that a malignant lesion is either low risk or high risk for recurrence27–28.
These include the location and size of the lesion, rate of growth, regular or irregular borders, presence of chronic inflammation, prior irradiation, or neurological symptoms. Clinical diagnosis may need to be confirmed by biopsy. A number of biopsy techniques exist, including shave, punch, incisional, or excisional. Shave biopsies may allow confirmation of diagnosis, but the other techniques give more useful information about the behavior of the tumor in the deeper dermis. Where an attempted excisional biopsy is inadvertently incomplete, identification of the residual disease may be difficult. For these reasons, if biopsy is to be performed prior to definitive treatment, a punch or an incisional biopsy technique is preferred. There are also histological features which are associated with the rate of tumor recurrence. These include degree of differentiation, lymphovascular or perineural invasion, tumor subtype, and depth of invasion27–28. Using these guidelines the National Comprehensive Cancer network has made available guidelines for the management of NMSC. Similarly the Australian Cancer Network, with funding from the Australian Government, and the National Health and Medical Research Council have also published comprehensive multidisciplinary guidelines for the management of NMSC29.
Management
Prevention
Given that sun exposure is one of the main precipitants of NMSC, measures to reduce exposure are very important. Sunscreen has been shown to reduce the incidence of SCC and precursors. Sun exposure should be avoided between 10.00 hours and 14.00 hours, when 60% of the most harmful UV exposure occurs. Application of 30 sun protection factor (SPF) sunscreen should occur prior to sun exposure and be repeated after swimming, or sweating. A broad-brimmed hat and clothing that does not transmit light should be worn outdoors. Additional exposure from solariums increases the incidence of BCCs, SCCs, and MM. Their use should be discouraged. Annually, 281 new melanoma cases, 43 melanoma-related deaths, and 2572 new cases of squamous cell carcinoma were estimated to be attributable to solarium use in Australia30–32.
α-difluoromethylornithine (DFMO) 10% ointment appears to reduce BCC incidence but not SCC incidence, and holds promise as a form of chemoprevention33–35.
Resveratrol
Resveratrol, a polyphenolic phytoalexin, is a chemopreventative agent, present in grapes and red wine, which is currently under investigation in animal studies. SKH-1 hairless mice exposed to UVB and treated with topical application of resveratrol had a statistically significant lower incidence of AK, IEC and SCC development36. Further studies have confirmed this chemoprevention of squamous skin tumor development in SKH-1 hairless mice and suggested that transforming growth factor β2 signaling is targeted37.
Afamelanotide (CUV1647) is an analog of α-MSH which promotes synthesis of melanin in cutaneous keratinocytes and melanocytes and is being evaluated for AK and SCC prevention in organ transplant patients38.
Investigation
The vast majority of periocular tumors need little or no investigation. Diagnosis is usually clinical and treatment can be instituted. There are, however, situations where investigations are necessary. Where a diagnosis is unclear clinically, biopsy can be helpful in order to plan management39. For most NMSC a shave or punch biopsy from the thickest or most representative tumor region can be performed. When radiotherapy is considered as primary treatment for selected cases (too frail for surgical excision, or other specific reasons) biopsy should be performed prior to treatment to confirm diagnosis and plan treatment.
Should a lesion have any clinical sebaceous features, as suggested by location, a diffuse lid margin thickening or yellowish discoloration, generous biopsy to include representative tissue sampling is important and some advocate full-thickness biopsy for this reason. Where a melanoma is suspected, ideally biopsy should be excisional. Shave or punch biopsies may result in incorrect diagnosis or errors in pathological staging, particularly in relation to tumor thickness40–42.
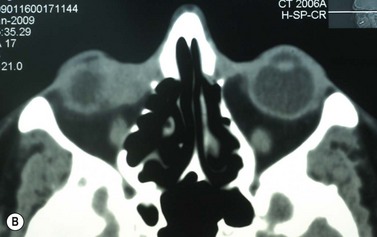
Where a lesion might have invaded the orbit, as suggested by tumor extent, limited eye movements, or enophthalmos, imaging is mandatory to look for the posterior extent of the tumor (Fig. 49.6). Where there might be a possibility of perineural invasion (PNI), imaging is important to obtain preoperatively, if possible. Should PNI be found on histology, imaging should be considered, depending on the size of nerves involved. PNI of small nerves within the excised specimen may be too small to detect with imaging. PNI of larger, named nerves seen on pathology, or patients with clinical evidence of PNI (cranial nerve palsies, altered sensation, pain), may be detected on imaging studies43–47.

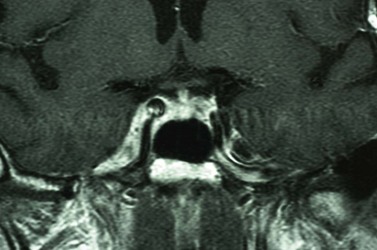
Magnetic resonance imaging (MRI) has better resolution for intraorbital structures and should be used for detection of PNI (Fig. 49.7). Larger tumors are also more likely to have PNI and imaging could be considered. Usually PNI will involve either motor or sensory nerve of the face and within the orbit coursing posteriorly to the brainstem. The possibility of PNI should be included on the imaging request form47.
Management of established disease
Once a tumor has developed and a diagnosis has been established, treatment should be undertaken to eradicate the tumor with minimal damage to surrounding ocular and periocular structures and their function. Currently available treatments for periocular tumors include surgery, radiotherapy, cryotherapy, curettage/diathermy, electro-dissection, photodynamic therapy, and topical agents (imiquimod, 5-fluorouracil, diclofenac gel), as well as emerging medical treatments. Traditionally, for most eyelid malignancies, the treatment has been surgical with excision of the tumor and subsequent repair. Less commonly, some lymphoid, metastatic or other lesions have are managed differently with chemotherapy, radiotherapy, or immunotherapy, reflecting their different tumor biology. The tumor should be staged according to the American Joint Committee on Cancer (AJCC) Eyelid Carcinoma staging protocol, which has been recently revised48. Further, if a melanoma, the AJCC specific melanoma staging system should be used49.
The integument consists of three main layers: the epidermis, the dermis, and the subcutis. The vast majority of cells are keratinocytes, involved in a staged maturation from the basal to superficial skin layers. Other cell types (<5%) include Langerhans cells, which have an important immune function, neural crest derived melanocytes, which are essentially protective, Merkel cells, which perform specialized sensory functions, as well as T-cells50.
Skin homeostasis is mediated by two populations of progenitors: renewable stem cells and their offspring, transient amplifying cells, which can give rise to the various cells of the hair follicle, the interfollicular epidermis (IFE), as well as sebocytes and sebaceous glands. The basal cells undergo an orderly, progressive maturation to suprabasal (or spinous cells), then granular cells. They then undergo a terminal differentiation into the stratum corneum, performing a barrier function before being shed as squames. Under the influence of lower levels of β-catenin they may develop into sebocytes and IFE, rather than hair follicles, suggesting that these pathways are closely linked51–52. Melanocytes migrate from the neural crest to the basal layer of the epidermis, uveal, and meningeal tissues, as well as ectodermal mucosa.
There are a number of important embryonic signaling pathways that influence skin development and homeostasis, influenced by a molecular conversation of their various proteins and genes. The most important of these are the hedgehog pathway (Hh), Wnt (wingless related mouse mammary tumor virus integration site), BMP (bone morphogenic protein), and notch53. Hh signaling influences hair follicle bulge stem cells to produce transit amplifying cells. This process is modulated by Wnt, which increases nuclear β-catenin resulting in upregulation of Hh signaling and Patched homolog 1 (Ptch1) in new follicles. Altered Hh function has been implicated in all BCCs following the finding of a mutant Ptch1 gene in the basal cell nevus syndrome (BCNS or Gorlin’s syndrome). Ptch1 functions as a classic tumor suppressor gene and 90% of sporadic BCCs can be shown to have Ptch1 mutations. Smoothened (SMO) is a downstream activator of the Hh pathway which may show an activating mutation in the remaining 10% of BCCs. Smo activates the Gli family of transcription factors. While genetic abnormalities at these levels are the most common seen in BCC development, other genes including those that influence skin color, repair DNA, or are involved with Wnt, PI3K, and FOXM1 have also been implicated.
SCC conforms to the multi-stage model of cancer, with mutations arising in the p53 tumor suppressor gene. Keratinocytes with multiple p53 mutations do not undergo apoptosis but rather proliferate with clonal expansion leading to SCC in situ and with progression to invasive SCC54.
MM progression from normal melanocytes has been linked to mutations in a number of genes involved: signaling RTK, Pl3K, retinoblastoma, p53, Wnt, and NF-kB pathways55. Five main oncogenes have also been implicated: NRAS, BRAF, MITF, NEDD-9, and KIT, and many others may also be involved.
Sebaceous carcinoma may develop via a number of different pathways. Muir–Torre syndrome is an autosomal dominant genodermatosis caused by mis-sense mutations in genes coding for mismatch repair enzymes, which is the best understood56. Loss of the fragile histidine triad protein has been shown to play a role in some periocular sebaceous carcinomas. Lef-1 mutations, as well as overexpression of β-catenin in the cytoplasm of eyelid sebaceous carcinomas have been reported, suggesting the involvement of multiple developmental pathways56–58.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


