37
The First Anti-VEGF Therapy: Pegaptanib Sodium
Anthony P. Adamis
INTRODUCTION
Until recently, the treatment of ocular neovascular diseases such as age-related macular degeneration (AMD), diabetic retinopathy (DR), and retinal vein occlusion (RVO) has been restricted to ablative laser-based procedures and surgical interventions. More than a decade of research has identified a central role for vascular endothelial growth factor (VEGF) in the etiology of these diseases, resulting in revolutionary new treatments based on inhibiting VEGF. Two anti-VEGF agents are approved as intravitreal therapies for neovascular AMD. Pegaptanib sodium, the first approved agent, is an RNA aptamer that binds the VEGF165 isoform while ranibizumab is a monoclonal antibody antigen-binding fragment that binds all VEGF isoforms. Bevacizumab, a related monoclonal antibody, also is being evaluated for the treatment of ocular neovascular diseases in off-label studies. This chapter will focus on the development and clinical application of pegaptanib.
VEGF AS A THERAPEUTIC TARGET IN OCULAR NEOVASCULAR DISEASE
The importance of VEGF in ocular neovascular diseases stems from its key properties as a regulator of physiological and pathological angiogenesis (1) and as a potent promoter of vascular permeability (2). As such, it contributes to two proximate causes of vision loss: the growth of aberrant retinal vasculature and macular edema. Clinical studies established that vitreous levels of VEGF were elevated in a number of ocular neovascular conditions (3–6) while preclinical work with several animal model systems demonstrated that such elevations were both necessary and sufficient for the development of ocular neovascularization (7, 8). Studies using animal models of diabetes also were important in establishing the role of VEGF in promoting the increased retinal leukostasis characteristic of DR believed to mediate much of the damage to the retinal vasculature associated with this disease (9).
Alternative splicing of the VEGF gene generates six principal isoforms (1, 10) with VEGF165 and VEGF121 being the most common variants in normal eyes (11). Preclinical evidence suggests that VEGF165 is especially pathogenic in that it was dramatically upregulated in a rodent model of ischemic neovascularization (12) and had more potent proinflammatory properties than VEGF121 (13). Such properties included chemoattraction of monocytes (13), which amplifies neovascularization induced by ischemia (12) or laser wounding (14–16), and upregulation of retinal expression of intercellular cell adhesion molecule-1 (13), a mediator of retinal leukostasis in DR (9). These data suggested that specific inactivation of VEGF165 could significantly ameliorate the effects of VEGF in ocular neovascular diseases. This concept was supported by two key preclinical observations in rodent models: not only was intravitreal pegaptanib as effective as a VEGF-receptor (R)-Fc fusion protein that binds all VEGF isoforms in suppressing ischemic ocular neovascularization (12) but it was also capable of reversing the diabetes-induced breakdown of the blood-retinal barrier (17).
VEGF exerts a wide range of actions both in the eye, where it is important in the maintenance of retinal neurons (18) and the choriocapillaris (19), and in the nervous system, kidney, bone, and liver (9, 20, 21). Furthermore, the aberrant neovasculature found in AMD and DR is especially permeable, increasing the potential for systemic exposure to intravitreal anti-VEGF agents (22), as evidenced by the detection of therapeutic effects in the fellow eyes following anti-VEGF therapies in DR (23) and AMD (24). The safety of nonselective versus selective anti-VEGF therapies will be explored in the clinical section of this review.
DEVELOPMENT OF PEGAPTANIB AS AN ANTI-VEGF OCULAR THERAPEUTIC AGENT
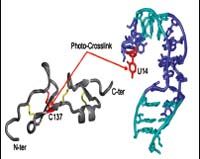
Pegaptanib is an RNA aptamer that was developed through three applications (25–27) of the SELEX [systematic evolution of ligands by exponential enrichment] procedure (28, 29) using VEGF165 as a target. Chemical modifications of the constituent nucleotides were used to improve its nuclease resistance and affinity, and two 5′ polyethylene glycol substituents were added to increase bioavailability (30). Pegaptanib was found to block the binding of VEGF165 to endothelial cell receptors, to inhibit VEGF165-mediated cell signaling and proliferation (31), and to reduce VEGF165-induced vascular permeability (27, 32) while not affecting responses to VEGF121 (31). Pegaptanib’s selectivity for VEGF165 derives from its interaction with the heparin-binding domain of VEGF165 (33), which is not present in VEGF121 (10). The predicted secondary structure of pegaptanib and its interaction with the heparin-binding domain of VEGF165 are shown inFigure 37-1(30).
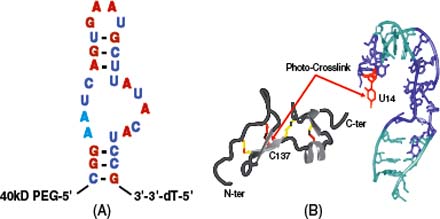
Figure 37-1. A: The sequence and predicted secondary structure of pegaptanib with 2′-O-methylated purines shown in red, 2′-fluorine-modified pyrimidines shown in blue, and unmodified ribonucleotides shown in black. The nucleotide modifications were made to increase bioavailability. The site of attachment of a 40 kDa polyethylene glycol (PEG) moiety is shown. B: The interaction between the 55 amino acid heparin-binding domain of VEGF165 and pegaptanib. The free heparin-binding domain of VEGF165 is shown in gray with disulfide bonds in yellow. Pegaptanib is shown in teal, with the interaction between cysteine-137 of VEGF165 and uridine-14 of the aptamer indicated in red. (Reproduced from Ng EW, Shima DT, Calias P, et al. Pegaptanib, a targeted anti-VEGF aptamer for ocular vascular disease. Nat Rev Drug Discov 2006;5:123–132, with permission.).
Initial pharmacokinetic studies of pegaptanib performed in monkeys found mean half-lives after intravitreal and intravenous administration of 94 hours and 9.3 hours, respectively, suggesting that clearance from the eye is rate-limiting; pegaptanib remained fully active in VEGF-binding assays 28 days after intravitreal injection (34). A subsequent clinical study of pegaptanib pharmacokinetics following intravitreal injection evaluated 147 patients with neovascular AMD who received either 1 mg or 3 mg every 6 weeks for 54 weeks (35). Mean maximal plasma concentrations in the 1 mg group ranged from 20 to 24 ng/ml; pegaptanib remained above the level of detection (8 ng/ml) for 1 week with a plasma mean terminal half-life of 10 days. Repeat injections did not result in any plasma accumulations nor were there detectable serum antibodies to pegaptanib (35).
Efficacy and Safety of Pegaptanib in the Treatment of Neovascular AMD
The efficacy and safety of pegaptanib for the treatment of neovascular AMD was established in the pivotal V.I.S.I.O.N. (VEGF Inhibition Study in Ocular Neovascularization) phase 2/3 trials (36). These two concurrent, multicenter, randomized, sham-controlled, dose-ranging trials enrolled subjects with all angiographic subtypes of neovascular AMD and lesions ≤12 disk areas. Subjects were randomized to receive intravitreal pegaptanib (0.3, 1, or 3 mg) or sham injections every 6 weeks for 54 weeks. For subjects with predominantly classic lesions, photodynamic therapy (PDT) with verteporfin was administered at the investigator’s discretion. The primary endpoint was the proportion of subjects losing <15 letters of visual acuity (VA); secondary endpoints included proportions gaining ≥0, ≥5, ≥10, or ≥15 letters, proportions losing ≥30 letters, mean changes in VA, and proportions progressing to legal blindness (VA 20/200 or worse) in the study eye. Of 1208 subjects enrolled, 1186 (98%) received at least one treatment (mean: 8.5 of a possible 9 injections) and were evaluated at week 54.
Efficacy of Pegaptanib
All pegaptanib doses proved superior to sham according to the primary endpoint. Compared to 55% of sham subjects, proportions losing <15 letters for the 0.3 mg, 1 mg, and 3 mg groups were 70% (p < .001), 71% (p < .001), and 65% (p < .03), respectively (36). As no further benefit accrued to higher doses, further analysis was restricted to the 0.3 mg dose. Pegaptanib was superior to sham for all secondary endpoints as well, including proportions losing ≥30 letters (10% vs. 22%, respectively; p < .001) or progressing to legal blindness (38% vs. 56%, respectively; p < .001), mean change in VA (−7.95 vs. −15.05 letters, respectively; p < .05), and gaining ≥0, ≥5, ≥10, or ≥15 letters (p < .05 for each comparison) as depicted inFigure 37-2(37). Subgroup analysis revealed that the treatment benefit was conferred irrespective of baseline VA, lesion size, angiographic subtype, sex, age, race, or iris color.
In the second year of the study, 1053 subjects were rerandomized for an additional 48 weeks, with 943 (90%) being evaluated at week 102 (38). Subjects receiving pegaptanib in year 1 were randomized either to the same dose or to discontinue treatment, while sham subjects from year 1 were randomized either to continue or discontinue sham or to switch to one of the three drug doses. Compared to those receiving sham for 2 years (including those discontinuing sham), subjects continuing 0.3 mg pegaptanib for 2 years received significant clinical benefit according to the primary endpoint (45% losing <15 letters vs. 59%, respectively; p < .05). Subjects receiving 0.3 mg pegaptanib also had superior outcomes in terms of mean VA, likelihood of progressing to legal blindness, and proportions gaining vision compared to subjects receiving usual care. Moreover, a higher proportion of those continuing treatment for 2 years had a <15 letter loss compared to those who discontinued treatment in year 2 (38).
A further exploratory subgroup analysis of the V.I.S.I.O.N. data was also conducted to assess whether pegaptanib had benefits in treating earlier stage lesions (39). Two subgroups were defined as exemplifying early disease based on criteria such as baseline lesion size, lack of prior PDT, absence of classic lesions, and absence of lipid. For these two groups, proportions losing <15 letters were 76% and 80% among subjects receiving 0.3 mg pegaptanib compared with 50% and 57% for the sham group (p ∇ .03 and p ∇ .05, respectively); in addition, sham-treated subjects were approximately 10 times more likely to progress to legal blindness. Despite the relatively small size of the subgroups included in this analysis, these results suggest that earlier treatment of AMD with pegaptanib may result in superior vision outcomes (39). Very similar conclusions recently were reported from a retrospective study of 90 subjects receiving pegaptanib as primary therapy, where the proportion of subjects losing <15 letters was 90% (40).
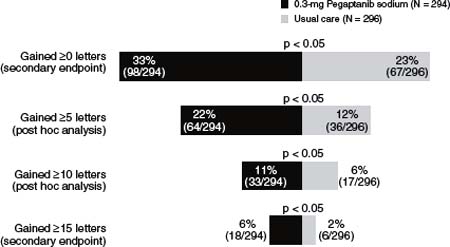
Figure 37-2. The proportion of subjects who maintained or gained visual acuity at 54 weeks in the V.I.S.I.O.N. (VEGF Inhibition Study in Ocular Neovascularization) trials. (Reproduced from Ng EW, Adamis AP. Targeting angiogenesis, the underlying disorder in neovascular age-related macular degeneration. Can J Ophthalmol 2005;40:352–368, with permission.)
Data from the ranibizumab phase 3 trials in neovascular AMD strongly suggested that blockade of all VEGF-A isoforms is more effective than VEGF165 blockade alone. Where pegaptanib showed good efficacy was in preclinical models manifesting retinal ischemia and neovascularization, where VEGF165 was the predominant isoform. Thus, pegaptanib may show greater efficacy in DR and RVO. Conversely, retinal ischemia does not appear to be an important driver of choroidal neovascularization.
Safety of Pegaptanib
The long-term safety of pegaptanib has been established in more than 4 years of follow-up in the V.I.S.I.O.N. trials (36, 41–43). Injection-related events such as endophthalmitis, cataract, and retinal detachment were rare, and prolonged treatment with pegaptanib was not found to have detrimental effects on the retinal pigment epithelium (RPE) or on retinal neurons (44). In a separate dedicated systemic safety trial, 147 subjects with neovascular AMD received 1 mg or 3 mg pegaptanib every 6 weeks for 54 weeks (3 to 10 times the clinical dose), and no systemic safety signals were detected (35). There have been occasional postmarketing reports of RPE tears with pegaptanib (45). A recent review found that reports of RPE tears following the administration of all three anti-VEGF agents occurred primarily in eyes with existing RPE detachments (46). There also have been rare instances of anaphylactoid reactions with pegaptanib therapy (47).
Since inactivation of VEGF has the potential for interfering with a wide range of physiological processes, there are concerns about the potential systemic effects resulting from intravitreally administered anti-VEGF agents. An analysis of data from the ranibizumab trials, which for the first time demonstrated a mean increase in vision for AMD subjects in a trial of anti-VEGF therapy (48, 49), found a significantly greater incidence of nonocular hemorrhage in those receiving ranibizumab (50). In addition, a preliminary analysis of the ongoing SAILOR trial has identified a significantly greater incidence of stroke (1.2% vs. 0.3%, respectively; p ∇ .02) between the 0.3 mg and 0.5 mg doses, prompting a physician advisory letter from the manufacturer (51). A subsequent analysis of the final 1-year SAILOR data (52) revealed, though, that while the stroke incidence was still higher in the 0.5 mg group (1.2% vs. 0.7%), this difference was no longer statistically significant. It remains to be established whether there is any trade-off between the greater efficacy of agents that inactivate all VEGF isoforms, such as ranibizumab, and the safety in selectively targeting VEGF165 with pegaptanib.
INVESTIGATIONAL STUDIES INVOLVING PEGAPTANIB
Pegaptanib is being investigated as a treatment for ocular diseases other than neovascular AMD, including diabetic macular edema (DME) and proliferative diabetic retinopathy (PDR), as well as macular edema secondary to central retinal vein occlusion (CRVO) and branch retinal vein occlusion (BRVO). Pegaptanib also is being evaluated for use in alternate approaches, such as pegaptanib maintenance therapy following induction with a nonselective anti-VEGF agent or in combination with other treatments.
DIABETIC MACULAR EDEMA AND PROLIFERATIVE DIABETIC RETINOPATHY
Photocoagulation until recently has been the standard of care for DME and PDR (9), with pars plana vitrectomy being used for those with serious complications of progressive retinopathy (53). However, the importance of VEGF in PDR pathogenesis was highlighted in a recent study in which high vitreous levels of VEGF were found to be a significant predictor of progression of PDR following vitreous surgery (54), supporting the investigation of pegaptanib for the treatment of ocular complications of diabetes.
The use of pegaptanib in the treatment of DME was evaluated in a phase 2, double-masked, multicenter, randomized controlled trial (55) in which 172 subjects with DME received intravitreal pegaptanib (0.3 mg, 1 mg, or 3 mg) or sham injections at baseline and at 6 and 12 weeks; additional injections, including the option of photocoagulation, were given through week 30 as needed, with final assessments at 36 weeks. Compared with sham, 0.3 mg pegaptanib resulted in significant clinical benefit according to all three prespecified endpoints, median VA (20/50 vs. 20/63, respectively; p ∇ .04), mean change in retinal thickness on optical coherence tomography (OCT) (−68 μm vs. ≶4 μm, respectively; p ∇ .02), and proportions requiring photocoagulation therapy (25% vs. 48%, respectively; p ∇ .04) (55).
Among subjects in the DME trial (56), there were 16 evaluable subjects with retinal neovascularization at the study entry; eight of 13 (62%) eyes receiving pegaptanib had complete regression of neovascularization at 36 weeks as assessed by fundus photographs, absence of leakage on fluorescein angiography or both. Cessation of treatment led to recurrence of the neovascularization in three of these eyes. Figure 37-3 shows an example of a case where regression of retinal neovascularization at week 36 was followed by the reappearance of neovascularization at week 52. There was no regression in any of the three sham-treated eyes with baseline neovascularization or in the four fellow eyes with neovascularization of subjects treated with pegaptanib. Similarly, in a pilot study of patients with PDR given pegaptanib every 6 weeks or panretinal photocoagulation (PRP) for 30 weeks with a final assessment at 36 weeks, eight of eight (100%) pegaptanib-treated patients showed complete regression of neovascularization (56). In contrast, only three of eight (38%) eyes treated with PRP had regression, with one eye developing vitreous hemorrhage and four of eight (50%) continuing to have active neovascularization at week 36 (57). The presence of retinal cysts did not appear to affect responses to pegaptanib, with similar improvements in VA and in center point thickness at week 12 or week 36 in patients with or without retinal cysts (58).
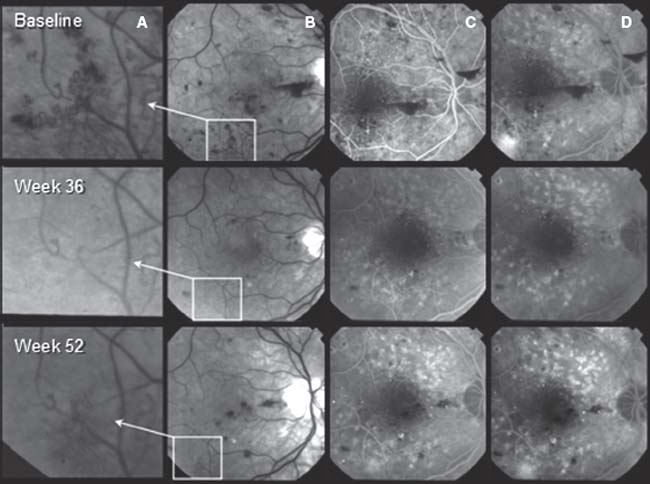
Figure 37-3. Subject 10. First row: Baseline visit shows a magnification of retinal neovascularization elsewhere (NVE) (A), the location of the neovascularization along the inferotemporal arcade (red-free photograph) (B), areas of capillary nonperfusion in the early-phase frame (fluorescein angiogram) (C), and leakage from the NVE in the late-phase frame (fluorescein angiogram) (D). Second row: At week 36, after six periodic pegaptanib injections and 6 weeks since the most recent injection, regression of NVE is seen on red-free photographs (A, B), lessening of apparent microaneurysms in the early phase (C), and regression of leakage from NVE in the late phase (D). Third row: Fifty-two weeks after study entry and 22 weeks since the last pegaptanib injection, the reappearance of NVE is seen on red-free photographs (A, B) as well as the reappearance of leakage from NVE in the early- and late-phase frames (C, D). (Reproduced from Adamis AP, Altaweel M, Bressler NM, et al. Changes in retinal neovascularization after pegaptanib (Macugen) therapy in diabetic individuals. Ophthalmology 2006;113:23–28, with permission.)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


