Purpose
To identify the major traction mechanisms that cause myopic traction maculopathy and to determine whether surgery can be tailored successfully to the specific mechanism involved.
Design
Nonrandomized, retrospective, interventional case series.
Methods
We performed a chart review of consecutive patients who underwent vitreoretinal surgery for myopic traction maculopathy by a single surgeon at a tertiary referral center. Traction mechanisms were identified based on preoperative and intraoperative findings and postoperative response to a tailored surgical approach.
Results
Six eyes of 6 patients with a minimum follow-up of 6 months were included. Major pathogenic traction mechanisms included perifoveal posterior vitreous detachment with vitreomacular traction in 3 eyes, noncompliance of native internal limiting membrane in 2 eyes, epiretinal membrane in 1 eye, and remnant cortical vitreous layer after posterior vitreous detachment in 1 eye. One eye exhibited 2 traction mechanisms. The surgical approach addressed only the major traction mechanism(s) identified in each eye. After surgery, the visual acuity improved by 2 lines or more in all eyes, and macular thickening resolved completely in 5 (83%) of 6 eyes and partially in the remaining eye.
Conclusions
The traction mechanisms causing myopic traction maculopathy are diverse. Vitreoretinal surgical repair for this condition is successful when the major traction mechanisms causing tautness of the inner retina are identified and relieved.
The term myopic traction maculopathy was used first by Panozzo and Mercanti to describe a collection of pathologic changes associated with highly myopic eyes, including macular retinoschisis, foveal detachment, and macular hole. Also known as myopic foveoschisis , these changes occur in approximately 8% to 34% of people diagnosed with pathologic myopia. Before the advent of optical coherence tomography (OCT), this disorder was difficult to diagnose, and surgery typically was performed for presumed foveal detachment or macular hole. As the resolution and the quality of OCT imaging have improved, so has the ability to understand the pathoanatomic features of this condition.
As suggested by the name myopic traction maculopathy , it is widely accepted that a pulling or stretching force is the primary pathologic mechanism in this disorder. The precise cause for this traction, however, is still debated. Arguments have been made for each of several preretinal structures as the source of traction, including a partially detached vitreous with vitreomacular adhesion, remnant cortical vitreous plaques after posterior vitreous detachment (PVD), and epiretinal membrane (ERM). Other authors, however, have argued that myopic traction maculopathy arises from elements intrinsic to the thinned myopic retina, including a taut internal limiting membrane (ILM) and shortened retinal arterioles, either of which could lead to tangential traction and various pathologic consequences.
The lack of consensus for a single pathophysiologic mechanism has spawned a similar debate regarding the best surgical approach for treatment of this condition. Major areas of controversy include the role of intravitreal gas after vitrectomy and the need for ILM removal. To date, no report has sought to illustrate the multiple tractional elements that can lead to myopic traction maculopathy while demonstrating a similar diversity of successful surgical approaches. Herein, we describe the major traction mechanisms that cause myopic traction maculopathy and demonstrate that surgery can be tailored successfully to the specific pathologic mechanism involved in a given eye.
Methods
We performed a retrospective review of the medical records, OCT images, and color fundus photographs of consecutive patients who underwent vitreoretinal surgery for myopic traction maculopathy by 1 surgeon (M.W.J.). Patients were considered to have myopic traction maculopathy if, in addition to high myopia, they had diffuse schisis-like retinal thickening throughout the macular area confirmed by OCT. All patients were examined, diagnosed, and operated on at a large academic tertiary care center between 2001 and 2009. The minimum period of postoperative follow-up for inclusion in this study was 6 months. No patient meeting these criteria during this period was excluded.
OCT was performed through a dilated pupil by a certified ophthalmic photographer using commercially available equipment (Stratus OCT III or Cirrus HD-OCT; Carl Zeiss Meditec, Inc, Dublin, California, USA). The OCT studies comprised scans 6 to 9 mm in length, oriented either as 6 radial lines at intervals of 30 degrees (Stratus OCT) or as 5-line horizontal and vertical raster scans (Cirrus HD-OCT). Each OCT study was centered on the foveola. Preoperative vitreous status was determined by biomicroscopic examination (presence or absence of Weiss ring) combined with OCT images. PVD was staged as described previously. Macular traction mechanisms were identified based on preoperative and intraoperative findings and postoperative response to a tailored surgical approach. Anatomic resolution was defined as the disappearance of schisis-like retinal thickening as observed on OCT images obtained at postoperative follow-up visits.
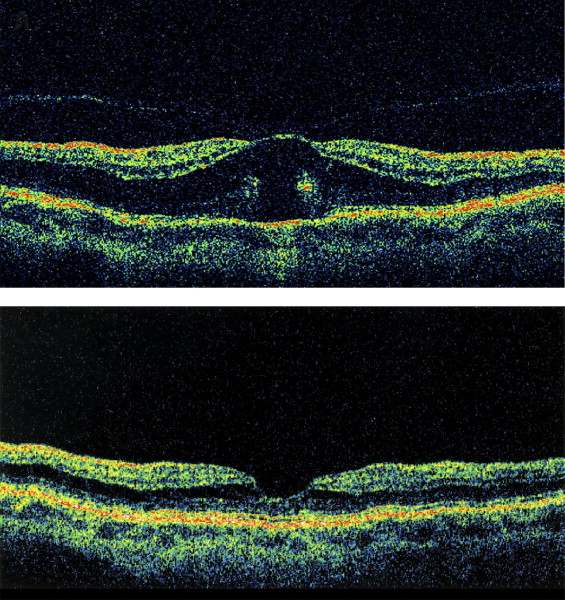
Case 1
A 52-year-old woman with a history of radial keratotomy surgery had an abrupt decrease in vision in her right eye to 20/200. The axial length in the right eye was 25.9 mm and the refractive error before radial keratotomy was unknown. Fundus and OCT examinations showed diffuse thickening of the outer macula and a stage 1 (perifoveal) PVD with a stage 1B macular hole. There was no clinically apparent posterior staphyloma. After core vitrectomy, a PVD was induced, including careful separation of the vitreous from the fovea. Examination of the retina around the fovea with a diamond-dusted membrane brush revealed no cortical vitreous remnants or ERM. Fluid–gas exchange was performed using 12% C 3 F 8 gas. The macular hole and macular thickening resolved by 4 months after surgery, and the visual acuity improved to 20/20 by 18 months after surgery. The eye remained stable through 27 months of follow-up ( Figure 1 ) .
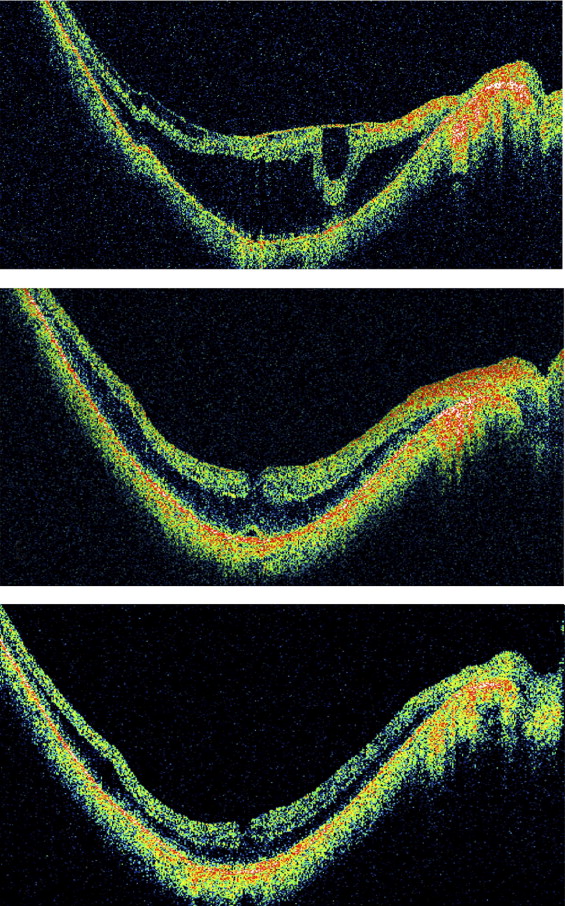
Case 3
An 81-year-old man sought treatment for a decrease in visual acuity in the left eye to 20/70 with a best correction of −10.00 diopters (D). Fundus examination and OCT of the left eye showed a Weiss ring, an obvious ERM, and prominent schisis-like macular thickening throughout a posterior staphyloma. During vitrectomy, a complete PVD was confirmed and the ERM was peeled. Neither ILM peeling nor intravitreal gas were used. The macular thickening resolved by 3 months after surgery, with visual recovery to 20/20 by 8 months. Seventy-two months after surgery, the eye was stable ( Figure 2 ).
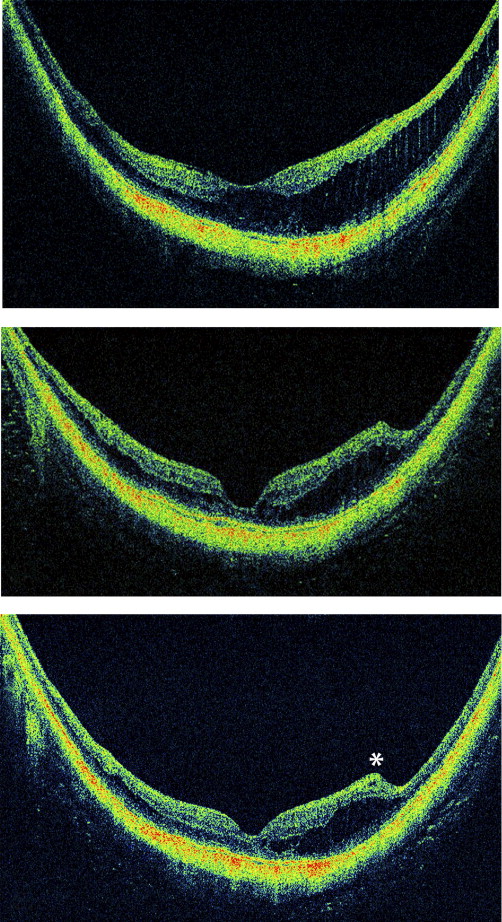
Case 4
A 62-year-old woman sought treatment for symptoms of worsening vision, metamorphopsia, and micropsia in the left eye. The past ocular history was notable for high myopia (−22.50 D), amblyopia, and esotropia in the affected eye. The visual acuity was 20/80 in the left eye. Fundus examination revealed a Weiss ring and schisis-like thickening within a posterior staphyloma. OCT demonstrated schisis-like macular thickening with traces of a thin preretinal membrane that was invisible clinically. During vitrectomy surgery, triamcinolone was used to identify and to help remove a broad and thin preretinal tissue layer from the macular region and extending into the retinal periphery. The peeled tissue had physical characteristics most consistent with vitreous cortex. Intravitreal gas (10% C 3 F 8 ) was used. After 6 months, the visual acuity had improved to the baseline of 20/60, and the symptoms of metamorphopsia and micropsia resolved. There was partial resolution of the schisis-like thickening ( Figure 3 ) .
Case 5
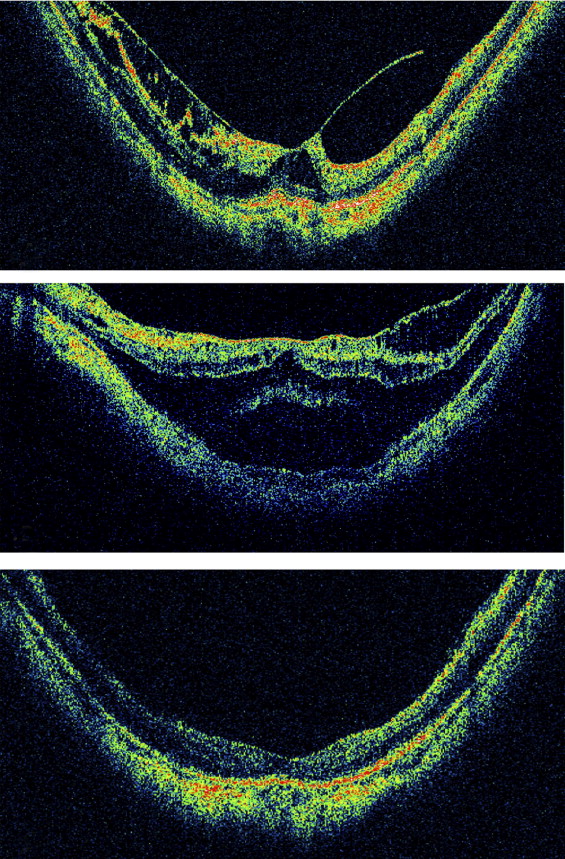
A 46-year-old woman sought treatment for increased metamorphopsia after slowly progressive vision loss in the left eye for 3 years. The refractive error was −13.50 D and the visual acuity was 20/80 in the left eye. Biomicroscopy demonstrated a posterior staphyloma and diffuse macular thickening. OCT examination showed schisis-like retinal thickening throughout the posterior staphyloma, with a localized vitreous detachment and no ERM. After surgical induction of a complete PVD during vitrectomy, triamcinolone was used to confirm that no cortical vitreous remnants were present on the retinal surface. The ILM was peeled and 5% C 3 F 8 gas was placed in the eye. The macular thickness resolved slowly over 6 months and acuity improved to 20/25 by 10 months after surgery. The eye remained stable through 35 months after surgery ( Figure 4 ) .
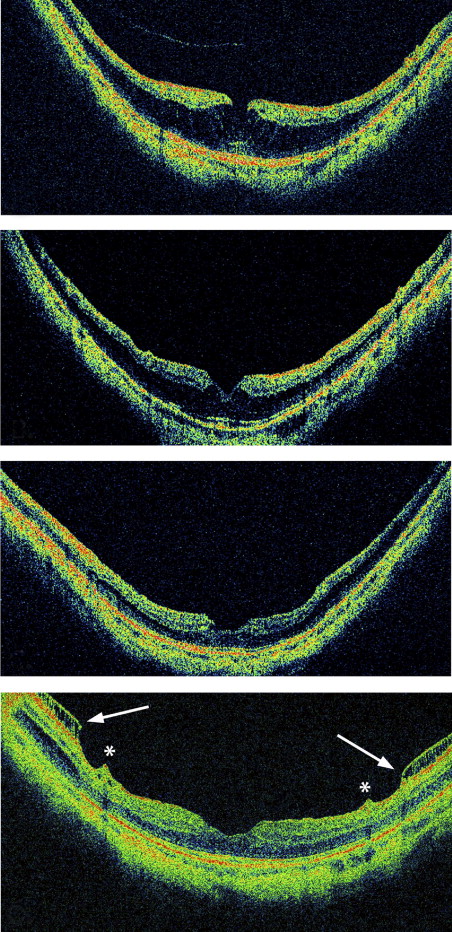
Case 6
A 48-year-old woman with a −15.50 D spectacle correction sought treatment for gradually progressive vision loss in the left eye. The visual acuity was 20/50. Fundus examination and OCT imaging demonstrated partial PVD with vitreomacular traction causing schisis-like thickening of the macula within a posterior staphyloma. She underwent vitrectomy with peeling of the posterior cortical vitreous. Four months after surgery, the visual acuity measured 20/80, the schisis-like thickening persisted, and a foveal detachment was evident on OCT. During a second vitrectomy, triamcinolone dusting revealed only a few small remnant cortical vitreous plaques on the macula, which were removed easily with a diamond-dusted brush. Because these isolated remnants were not believed to be relevant tractionally, the ILM was peeled and 10% C 3 F 8 gas was placed in the eye. Anatomic recovery occurred within 1 month and the visual acuity improved to 20/20 within 7 months after the second operation. These findings remained unchanged at last follow-up, 32 months after surgery ( Figure 5 ) .
Results
The study cohort included 2 men and 4 women with a mean age of 58.1 years (range, 46 to 81 years) at the time of surgery ( Table 1 ). Features of myopic traction maculopathy were unilateral in all patients. Five of the 6 (83%) study eyes had an obvious posterior staphyloma and high myopia of −10.0 D or more. The remaining eye had an axial length of 25.9 mm, no clinically evident posterior staphyloma, and a refractive error that was unknown because of previous radial keratotomy surgery. In addition to diffuse schisis-like thickening in the outer macula, associated findings included inner retinal schisis in 3 (50%) eyes, foveal detachment in 1 (17%) eye, and stage 1B macular hole in 1 (17%) eye. The preoperative vitreous status for each patient is listed in Table 1 .
| Patient | Age at Surgery (y) | Sex | Eye | MR (D)/Axial Length (mm) | Symptom Duration (mos) | PVD Stage | Staphyloma | Associated Findings | Preoperative VA |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 52 | F | Right | NA/25.9 | 2 | 1 | No | Stage IB MH | 20/200 |
| 2 | 60 | M | Left | −18.25/NA | 6 | 1 | Yes | Inner retinal schisis | 20/100 |
| 3 | 81 | M | Right | −10.00/29.19 | 92 | 4 | Yes | Inner retinal schisis | 20/70 |
| 4 | 62 | F | Left | −22.50/NA | 81 | 4 | Yes | None | 20/80 |
| 5 | 46 | F | Left | −13.50/NA | 36 | 2 | Yes | None | 20/80 |
| 6 | 48 | F | Left | −15.50/27.91 | 1 | 1 | Yes |
|
|
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


