13
The Diagnosis and Surgical Management of Dizziness and Vertigo
The indications for surgery of dizziness/vertigo are often empirical and ill defined. Nevertheless, surgery has a definite place in the overall management of patients with vertigo provided that the exact cause of the symptoms is accurately established. This is best achieved by developing a clear understanding of the mechanisms by which balance is maintained. The surgeon should also have an excellent grasp of the scope, sensitivity, specificity, and relevance of a wide spectrum of diagnostic tests commonly used in evaluating patients with dizziness. This chapter presents these foundational principles and discusses their practical application with illustrative case reports. The surgical techniques used will be described in brief, and the possible risks and complications and their prevention discussed.
■ Mechanisms for Maintenance of Balance
Balance is maintained by the central integration of sensory inputs from the visual, vestibular, and proprioceptive systems. After analysis of this information and comparison with previous experience, a coordinated motor output is initiated. Regardless of the system affected, patients invariably complain with the generic term dizziness. The task of the physician is to detect the system in which the abnormality resides and to investigate the affected system thoroughly. As otolaryngologists, our interest and expertise are in the vestibular system, and as such, a clear understanding of this system will help in reaching a correct diagnosis and instituting proper management. If the underlying disorder is suspected in the other systems, consultation should be sought. It is particularly important to reach a correct diagnosis if surgical treatment is planned because inappropriate management can have permanent and disastrous consequences for the patient.
In the absence of movement and in the anatomical position, a symmetrical, steady spike discharge is generated by each labyrinth. These discharges travel along the vestibular nerves to the ipsilateral vestibular nucleus. In mammals the rate of these discharges is estimated to be 90 impulses per second. Afferents from the horizontal semicircular duct synapse with neurons located in the ipsilateral vestibular nucleus. Second-order postsynaptic fibers travel in the medial longitudinal fasciculus (MLF) to the contralateral abducens nucleus. After a second synapse in the sixth nerve nucleus, the third-order neurons travel to the contralateral lateral rectus muscle. A second set of vestibular nuclear postsynaptic afferent fibers connects with the contralateral accessory abdu-cens nucleus neurons. The postsynaptic fibers then travel in the MLF to the ipsilateral oculomotor nucleus. After a third synapse, these fibers go on to innervate the ipsilateral medial rectus muscle (Fig. 13–1) In the case of the superior semicircular duct, the first synapse is in the vestibular nucleus. The second-order neurons travel up in the MLF to the opposite third nerve nucleus. Third-order neurons cross the midline and innervate the ipsilateral superior rectus muscle (Fig. 13–2). A second set of-third-order neurons go on to innervate the contralateral inferior oblique muscle.1
Afferents from the posterior semicircular duct also synapse in the ipsilateral vestibular nucleus. One set of second-order neurons ascend in the MLF to the opposite third nerve nucleus. After synapse, the third-order neurons go on to innervate the opposite inferior rectus. A second set of vestibular efferent neurons also ascend in the MLF, cross the midline, and synapse in the opposite fourth nucleus. Third-order neurons cross the midline and innervate the ipsilateral superior oblique muscle (Fig. 13–3).1
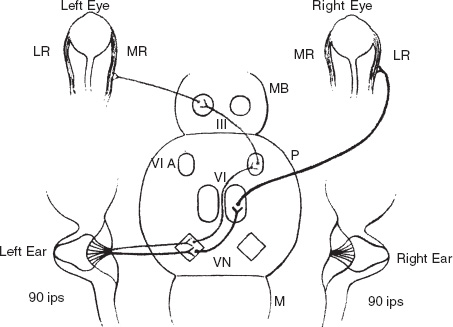
FIGURE 13-1 Neural connections of the crista ampularis of the left horizontal semicircular duct. VN, vestibular nucleus; M, medulla; P, pons; MB, midbrain; MR, medial rectus; LR, lateral rectus; VI, abducens nucleus; VI A, accessory abducens nucleus; III, oculomotor nucleus.
For an easy understanding of the neurophysiology of the vestibular system, only the changes that occur (with movement) in the lateral semicircular duct (LSCD) will be described. Ewald’s laws, which accurately describe the function of the semicircular canals, are significant. His first law states that induced nystagmus always occurs in the plane of the stimulated semicircular canal. Thus caloric stimulation, which primarily affects the LSCD, causes a horizontal nystagmus. Ewald’s second law states that in the LSCD, utriculofugal deflection of the cupula (i.e., deflection of the cupula away from the utricle) causes a decrease in the spike discharge from the crista ampularis, whereas a utriculopetal deflection of the cupula (i.e., deflection of the cupula toward the utricle) causes an increase in the spike discharge. Cold caloric stimulation of the right ear causes a utriculofugal deflection of the cupula, and thus there is a reduction in the spike discharge. The opposite pathway becomes the dominant tract, resulting in a contraction of the left medial rectus and the right lateral rectus. Thus the eyes tend to drift toward the right ear. When the limits of eye rotation are reached, the fast component of the nystagmus is initiated. This fast component would beat to the left. With warm caloric stimulation, the cupular deflection is utriculopetal, and the nystagmus beats toward the stimulated ear. Thus we can understand the mnemonic COWS (cold to the opposite, warm to the same) (Table 13–1; Figs. 13-4 and 13-5).
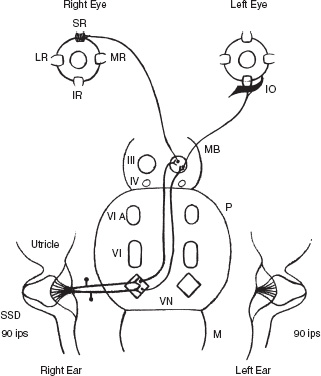
FIGURE 13-2 Neural connections of the crista ampularis of the right superior semicircular duct (SSD). SR, superior rectus; IO, inferior oblique; IR, inferior rectus; LR, lateral rectus; M, medulla; MB, midbrain; MR, medial rectus; P, pons; VN, vestibular nucleus; III, oculomotor nucleus; IV, trochlear nucleus; VI, abducens nucleus; VI A, accessory abducens nucleus.
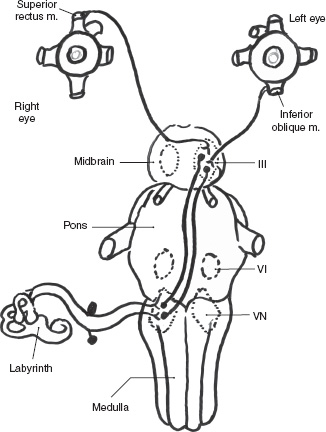
FIGURE 13-3 Neural connections of crista ampularis of the right posterior semicircular duct (PSD). VN, vestibular nucleus; III, oculomotor nucleus; VI, abducens nucleus.
By the same reasoning and with an appreciation of the vestibulo-ocular connections already described, the right-beating nystagmus caused by a destructive lesion of the left labyrinth can be understood. If both labyrinths are destroyed, as after treatment with ototoxic medications, the vestibular ocular reflex (VOR) is lost bilaterally and any head movement causes oscillopsia. Ewald’s third law states that in the vertical canals, utriculofugal deflection of the cupula causes an increase in the spike discharge, whereas a utriculopetal deflection causes a decrease in the spike output. The neural pathways for the vertical canal vestibulo-ocular pathway are different, and hence the direction of the nystagmus as in the superior semicircular canal syndrome is down-beating with positive pressure. With rotational testing, both labyrinths are stimulated at the same time. During clockwise rotation, the endolymph of the horizontal duct moves in an opposite, counterclockwise direction (because of its inertia), causing a utriculopetal deflection of the right cupula (i.e., a deflection of the cupula toward the utricle) and a utriculofugal deflection of the left cupula (i.e., a deflection of the cupula away from the utricle). The net result of such a stimulus is that the spike discharge from the right labyrinth is greater and, as already explained, a right-beating nystagmus results.
■ Assessment of Vestibular System Function
Traditionally, function of the vestibular system has been assessed by thermal stimulation of each labyrinth. The recording and quantification of the induced nystagmus provide a measure of the function of each labyrinth. Ideally the test results should also define the site of the lesion, whether labyrinthine or retrolabyrinthine (central). The Torok monothermal caloric test makes such a differentiation fairly accurately with three test results, namely, recruitment, decruitment, and hyperactivity. It is for this reason that the senior author (AK) prefers this technique of caloric stimulation, which has been described in previous publications.2 If two strengths of stimuli are applied to the same ear, and if the response to the stronger stimulus is disproportionately larger and the ratio is greater than 3.5, the test result is called vestibular recruitment. It is a sign of a labyrinthine lesion and the numeric values in such a patient could be as follows, indicating a lesion on the left side:
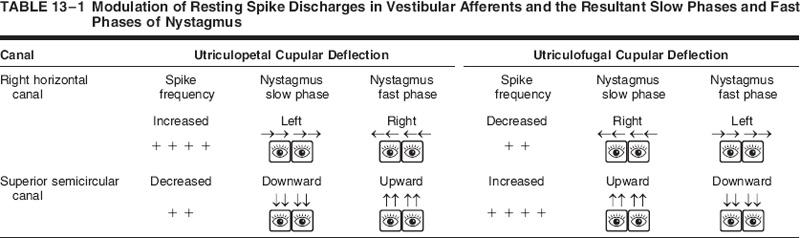
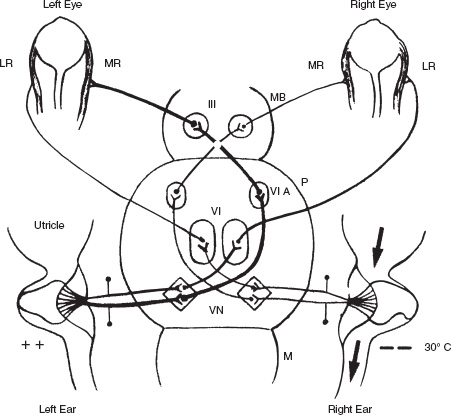
FIGURE 13-4 Cold caloric stimulation of the right ear. The endolymph flow is away from the utricle (arrow) and thus the cupular deflection is utriculofugal (away from the utricle). With the patient seated and the head extended, the horizontal canal is in the vertical plane. VN, vestibular nucleus; VI, abducens nucleus; VI A, accessory abducens nucleus; III, oculomotor nucleus; MR, medial rec-tus muscle; LR, lateral rectus muscle; M, medulla; P, pons; MB, midbrain.
10 mL: | 100 mL= | Ratio | |
|---|---|---|---|
Right | 15: | 30= | 2.0 |
Left | 10: | 40= | 4.0 |
On the other hand, if the response to the stronger stimulus is less than that obtained with the weaker stimulus, the test result is called vestibular decruitment, and it is a sign of a central lesion. The ratio in such a case is 1.1 or less, and the numeric values in such a patient could be as follows, indicating a left-sided lesion:
10 mL: | 100 mL= | Ratio | |
|---|---|---|---|
Right | 12: | 24= | 2.0 |
Left | 25: | 20= | 0.8 |
If the caloric responses to both the weak and the strong stimuli are greater than the mean normal values, the responses are considered hyperactive, and such a test result is interpreted to indicate a brainstem or cerebellar lesion. The values in such a case could be as follows:
10 mL: | 100 mL= | Ratio | |
|---|---|---|---|
Right | 43: | 90= | 2.0 |
Left | 48: | 93= | 1.9 |
The sensitivity of vestibular decruitment and hyperactivity for central lesions has been previously studied and reported.3 The site of the lesion can also be suspected from the history of the illness and from other supporting test results, and confirmed with appropriate imaging studies. The following case reports are illustrative.
Case Report 1
A 61-year-old man, a recent immigrant from India, gave a several-month history of drainage from the right ear and right otalgia. He had been treated with local antibiotic—steroid eardrops and intravenous antibiotics without resolution of symptoms. Shortly after discharge from his most recent hospitalization, the pain in the ear became severe, the existing hearing loss became profound, and he developed vertigo and a right facial paralysis. With these symptoms, the patient was transferred to the University of Illinois Eye and Ear Infirmary (AK) for further management. There was no past history of hospitalizations in India, and his general health had been good. Physical examination of the left ear showed a normal external auditory canal and an intact mobile tympanic membrane (TM). The right external canal lumen contained a scanty white discharge, and the posterior superior canal wall skin appeared thickened and edematous. The TM appeared thickened and erythematous, and a definite perforation could not be defined. A strong left-beating spontaneous nystagmus was observed, and the patient displayed a right infra-nuclear facial nerve paralysis. An audiometric evaluation showed deafness on the right side. A contrast-enhanced T1-weighed magnetic resonance imaging (MRI) scan showed an enhancing mass in the middle ear and mastoid. Abnormal enhancement of the right cochlea, vestibule, and semicircular canals was also noted. The facial nerve enhanced from the geniculate ganglion to the middle of its intrameatal course. The patient underwent a radical mastoidectomy, and extensive granulation tissue was removed from both the mastoid segment and the middle ear space. However, the fallopian canal, the stapes footplate, and the semicircular canals were intact, and thus the cause of the facial paralysis, deafness, and vertigo could not be established intraoperatively. Because the patient was already deaf, it was elected to disarticulate the stapes and examine the vestibule. This space was found to be full of pale granulation tissue, which also filled the lumina of the cochlea and semicircular canals. A labyrinthectomy was completed, and the facial nerve decompressed. Post-operatively, the patient developed a postauricular wound infection that grew Staphylococcus aureus and responded poorly to subsequent trials of erythromycin and cephalexin. In view of the persisting infection, a purified protein derivative (PPD) skin test was applied, and this proved to be strongly positive. Microscopic examination of the tissue removed from the labyrinth also showed evidence of acute and chronic inflammation with a preponderance of plasma cells. Tissue culture of the granulations from the middle ear and vestibule, however, failed to grow acid-fast bacilli. The patient received a 6-month course of isoniazid, rifampin, and pyrazinamide. On this treatment, there was complete resolution of the postauricular wound infection, and the facial nerve function returned to normal. For 4 years postoperatively, he had no further signs or symptoms of infection.
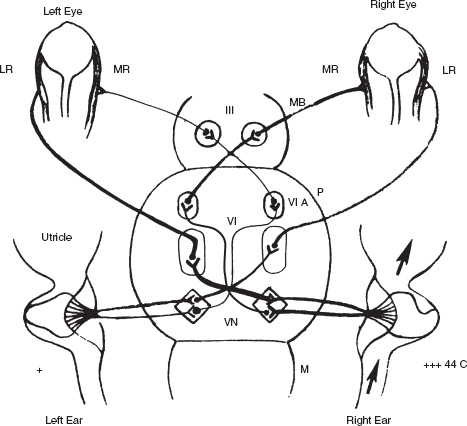
FIGURE 13-5 Warm caloric stimulation of the right ear. The endolymph flow is indicated by the arrows; the cupular deflection is toward the utricle. As with the cold caloric stimulation, the horizontal canal (with the patient seated and the neck extended) is in the vertical plane. VN, vestibular nucleus; VI, abducens nucleus; VI A, accessory abducens nucleus; MR, medial nucleus; LR, lateral rectus; M, medulla; P, pons; MB, midbrain.
Commentary
In this case the dizziness and the strong left-beating nystagmus were well explained by the fact that with destructive lesions of the vestibular end-organ, the spontaneous nystagmus beats away
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


