
Modern makeup artists exploit facial highlights by accentuating the subbrow area to “pop” with light colors. Further contrast is created by “shadowing” the pretarsal eyelid and medial canthus with smoky colors to create concavity and a sultry appeal (Fig. 38.3). Astute surgeons also recognize the effect shadows have on the aging face when attempting to re-establish youthful contours. Indeed, facial restoration has evolved beyond the purely excisional event wherein skin was removed to tighten the face. This older approach often yielded an unnatural “windblown” appearance after facial rhytidectomy. The study of facial shadows has led surgeons to replace volume in deficient areas while removing herniated or dependent tissue from other areas. Whether grafting fat or injecting fillers, the cosmetic surgeon must recognize the aged contours, as well as the aesthetically pleasing, youthful curves.

Fundamental Science
The cumulative effects of gravity, tissue laxity, fat redistribution, and generalized volume loss are all factors in the sequence of facial aging. The aging process is complex and involves both intrinsic and extrinsic factors.
Intrinsic factors are inherited genetic traits. To date, it has been understood that we have little control over our genes and must accept that we ultimately resemble our parents. Extreme aging is evident in progeria, a genetic disease that is heralded by rapid, irreversible, and accelerated aging.1,2 Afflicted individuals show premature signs of aging and have a shortened lifespan. The thin, sagging skin and bony face of an octogenarian can be present in a person as young as 8 years of age (Fig. 38.4). Certainly, learning about the genetics and pathophysiology of this debilitating condition will help elucidate the normal facial aging process.

Extrinsic factors are brought about by the environment and may be modified. These include stress, sleep, work, diet, weight loss, sun exposure, smoking, alcohol, drug use, and disease.3–5 On a microscopic level, there is cellular senescence, decreased proliferative capacity, decreased cellular DNA repair capacity and chromosomal abnormalities, hormone reductions, oxidative stress, and gene mutations.6 The deleterious effects of smoking and ultraviolet (UV) light have been well documented not only for their obvious effect on aging but also for their link to cancer7 (Fig. 38.5). UV light breaks down collagen and elastic tissue in the skin and causes damage at the cellular level. DNA is altered, causing free oxygen radicals that can damage and age the skin (Fig. 38.6). Smokers have long been known to have more facial lines consistent with a weathered face. The pathognomonic vertical smoker lines that ring the lips are a telltale sign of smoking, age, and poor health (Fig. 38.7). Nicotine narrows the blood vessels, limiting their carrying capacity for nutrients and compromising tissue integrity. The deleterious effects of both alcohol and nicotine, with advanced signs of perioral aging that manifest as decreased height of the vermillion border, lip rhytids, and sagging of the lips, are well documented.8



Two case series on identical twins shed light on facial aging and beauty. Identical twins illustrate the effects of genetic influence and help improve our understanding of environmental effects. One study on identical twins with disparate lifestyles9 (Fig. 38.8) found that the twin who had more sun exposure or who smoked had more facial lines and lid sagging and subjectively appeared older. Another study found that identical twins do not mature identically but develop subtle differences in features as they age. Facial symmetry is a major influence in attractiveness with aging, and factors such as sleeping position, dental history, and smoking all have an impact.10 Constant prone sleeping has been associated with a smaller, flatter side of the face, which creates facial asymmetry. Teeth extraction and noncompliance with denture wear also had a negative impact on facial growth as a result of less facial skeletal support and a smaller hemiface on the side of the extraction. Smoking causes aging and asymmetry as a result of the harmful chemicals in tobacco and also because people habitually smoke out of the same side of the mouth, which causes eventual asymmetry.

Clinical Features: Comparison of Youthful and Aged Facial Features
The aged face is characterized by several consistent features that transcend gender or culture and are summarized in Figure 38.9. One hallmark of a youthful face is the appearance of high cheekbones that gently taper to a defined jaw line. This is known as the “triangle of youth” and is drawn by a horizontal line between the cheek bone prominences forming the base with the apex of the triangle at the point of the chin. This heart shaped face can be seen in ages from the 20s to the early 50s, with a gradual loss of facial support and structure thereafter. In part as a result of the effects of gravity, this shape is ultimately replaced by the “pyramid of aging” when the triangle of youth flips over11,12 (Fig. 38.10). A horizontal line drawn between the jowl points forms the base, with the apex at the glabella completing this triangle. The facial morphology changes in part because of bone and tissue shifts with loss of volume in the cheeks and a new fullness in the jowls resulting from facial tissue descent and fat deposition in this area. One goal of aesthetic facial restoration, therefore, is to flip the pyramid of aging back to the triangle of youth.


A remarkable set of yearly photographs chronicling four sisters in the same position from 1975 to 2014 demonstrates the critical features of facial aging.13 The evolving female face has been marked by deterioration of soft tissue, with the most marked deflation occurring in the temporal, infraorbital, and cheek regions.14 A predictable pattern of the effects of aging on external facial features at various stages of life has long been recognized. In the fourth decade, the skin begins to sag; in the fifth decade, wrinkles and furrows appear; in the sixth decade, the lids become heavy, the nasal tip descends, and wrinkles become more prominent around the mouth and neck; in the seventh decade, the skin thins further and adipose tissue becomes less; in the eighth decade, facial wasting is more apparent and the malar mound is accentuated; and after 80 years of age, wrinkles become confluent, the skull size decreases, and the skin and subcutaneous fat diminish further15 (Fig. 38.11).

Pathogenesis of the Aging Face
Longitudinal studies have confirmed that facial aging stigmata are heralded by deepening of the facial folds, drooping of the upper lip, and increased projection of the lower eyelid.16 The surface changes reflect the alterations not only in the skin but also in the anatomic structures lying beneath it. The facial skeleton, facial muscle, fat, connective tissues, and skin all play a part in the transformation of the aging face.17,18 As craniofacial support (the table) shrinks with age, there is diminishing surface area for the overlying soft tissue covering (the tablecloth), exacerbating the sagging, particularly in the midface and perioral areas.19
Interestingly, the various components and tissues of the face do not age synchronously.20 The topographic appearance of the aging face results from a continual loss of volume and tissue descent caused by the unrelenting forces of gravity, loss of elasticity, and the wearing effects of chronic muscle movement (Fig. 38.12C).


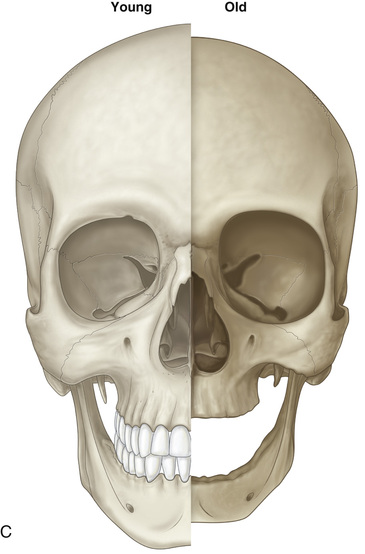
Facial Bones
Once perceived as static, the facial bones are now recognized to be in a state of flux. Just as the long bones in our bodies lose tensile strength and resorb over time, so do the facial bones. A decrease in facial height is seen as a result of atrophy of the mandible and the maxilla. Temporal hollowing from loss of bony support along with soft tissue and muscle atrophy contributes to a narrow, pinched-appearing upper face. The brows fall below the orbital rim because of loss of bony volume with subsequent lateral brow ptosis.21,22
Aeration of the sinuses in our facial skeleton plays an early role in facial bone remodeling. The ethmoid and maxillary sinuses, pea sized at birth, are the first to pneumatize. The maxillary sinuses grow in a biphasic manner between the ages of 0 and 3 years and again between 6 and 12 years. They become the largest sinuses, eventually achieving the pyramid-shaped cavities familiar on facial computed tomography (CT) scans. The frontal sinuses are not formed at birth and are the last to aerate but appear after age 4 years and grow rapidly after age 6 years until age 20 years.23 Maxillary sinus volume can decrease in older age, and osseous resorption can paradoxically cause enlargement of the frontal sinus.24,25 These factors contribute to the changes of the facial bones. The facial skeleton continues to remodel, eventually resulting in a clockwise rotation of the maxilla relative to the cranial base, with a posterior movement of the inferior maxilla and an anterior movement of the frontal bone26,27 (Fig. 38.13).

Many studies have demonstrated the topographic bony changes of the facial skeleton by using three-dimensional CT. Diagonal eye socket expansion occurs as a result of bony resorption. Initially round and small, the orbit enlarges to a tilted ovoid aperture with downward orbital rim remodeling28,29 (Fig. 38.14). The result is an orbital rim that expands superomedially and inferotemporally with age. This socket expansion also creates more depth to the socket, creating an intraorbital soft tissue volume deficit30 (Fig. 38.15). The orbital contents, including the globe, extraocular muscles, tendons, and fat, recede into the enlarging socket, giving a sunken, atrophic, aged appearance. The supporting orbital septa are adherent to the orbital bones, and their attachments to the soft tissue structures stretch over time. The attenuated septum allows fat to prolapse forward through a weaker retaining septal wall. The herniated fat presents as a bag or circle that creates a tired appearance. It is fascinating that the aging lower lid results more from a larger skeletal transformation than from prolapsed fat alone.


The bony changes continue into the midface, where the maxillary bone resorbs, repositioning the inferior orbital rim more posteriorly over time. The bony loss in this area can also be demonstrated with three-dimensional CT. A shrinking facial skeleton results in less support and projection of the overlying soft tissues. The corresponding soft tissues sag, contributing to the aged appearance. The result is less support in the midface and a decreased cheek projection. This is partially responsible for the hollowing in the midface and can create or accentuate a negative vector,31 an undesirable situation where the corneal apex projects anterior to the cheek in the sagittal plane. Patients with prominent eyes may have this trait, but midface deflation also contributes to this phenomenon.32
Loss of bony midface projection causes sinking of the cheeks and a longer lower lid. As more bone is lost in the midface, the lower lid is dragged inferiorly, which results in lengthening of the lower lid.
Bony changes around the eyes and cheeks also affect the overlying muscles that are attached to its surface. The upper lip elevators experience vector alterations with changes in their bony attachments. This contributes to loss of upper lip support, which leads to more lip wrinkles and allows the malar fat pads to slide downward, deepening the nasolabial folds.
The mandible also resorbs over time along with tooth loss, creating chin retrusion and weaker jaw projection.33 The loss of bony support creates further sagging of the overlying soft tissues and contributes to jowls and a poorly defined jaw angle. The oral cavity is also affected by loss of dentition and bone. The deficiency in structural support from tooth loss causes a general sinking in of the oral cavity and thus a gaunt appearance.
Facial Muscles and Ligaments
The muscles of facial expression and function also evolve with age, contributing to superficial aging changes. Mark Twain’s insightful comment “Wrinkles should merely indicate where smiles have been” underscores the origin of dynamic smile lines. Repetitive muscle contraction produces lines on the skin that are perpendicular to the muscle action. For example, chronic frontalis action to raise the brows causes horizontal wrinkles, and the horizontal movement of the corrugators causes the vertical “11” lines in the glabella. Hyperfunctional muscles that depress the brows, such as the corrugators, procerus, and the orbicularis oculi, gradually transform the dynamic lines into permanent, deep static rhytides and crevices. In essence, the muscles that act to raise the facial tissues are counteracted by muscles that depress the face. These agonist and antagonist muscle groups are constantly competing to establish facial balance, but with time, the muscles that depress the face win out. One example is in the upper face, where the only elevator is the frontalis muscle, counteracted by the numerous depressors of the orbicularis oculi, corrugators, procerus, and depressor supercilii. Injectable botulinum neurotoxins have become a successful means of treating these dynamic facial wrinkles and elevating the brows safely.
The repetitive contraction of the two facial sphincter muscles, the orbicularis oculi and the orbicularis oris, causes radial lines around the eyes and mouth, which become permanent over time. Contracture of the orbicularis oris, along with soft tissue atrophy, is responsible for the thinning of the lip with aging. These two flat sphincter muscles also weaken over time and can cause other facial changes. The orbicularis oculi stretches and elongates downward contributing to a longer lower lid34 (Fig. 38.16). Decrease in the thickness of the orbicularis oculi contributes to lower lid fat prolapse and the formation of “bags” under the eyes.35

Histologic studies have identified the mechanisms for the changing appearance of the lower eyelid. Findings of thinning of the middle portion of the orbicularis oculi, weakening of the midportion of the suborbicularis retaining fascia, decrease of the preseptal adipose tissue, distortion of the reticular cutis, and hanging down of the tarsal muscle all accompany aging and can partially explain progressive lower lid steatoblepharon (fat prolapse).36
This loss of muscle tone may also be partially responsible for malar festoons.37,38 These result from midface ligamentous changes. The firm orbicularis retaining ligament located below the inferior orbital rim stretches and lengthens over time, and its inferior descent eventually contributes to periorbital soft tissue ptosis.39,40 This ligament redrapes over the more resilient zygomatic cutaneous ligament, which lies directly below it and is the origin for many of the lip elevators such as the zygomaticus major, minor, and levator labii superioris. The result is a prolapse of tissue below the eye in the shape of a fluid-filled crescent defined by the subcutaneous ligaments.
The tear trough, a depression in the medial portion of the eyelid extending from the medial canthus to the midpupillary line, is another sign of aging. The tear trough is located between the palpebral and orbital portions of the orbicularis oculi muscle.41,42 The tear trough ligament is a fibrous osteocutaneous structure originating from the surface of the maxillary bone and extending through the junction of the palpebral and orbital portions of the orbicularis oculi muscle to attach into the skin.43 The appearance of the tear trough deformity can be attributed to subcutaneous tissue volume loss secondary to fat atrophy and malar descent.44
Another significant periocular aging change results from laxity of the lateral canthal tendons, with inferior and medial displacement.45 Tightening this structure re-establishes a youthful lid fissure and prevents functional lid malposition.
In the lower face, the orbicularis oris loses its tone, and the upper lip lengthens, accentuating upper lip ptosis and hiding the upper teeth, which contributes to the senile appearance. The depressor anguli oris causes turning down of the corners of the mouth and accentuates the “marionette lines” seen with aging.
The wide, flat platysma muscle derives its name from the Latin root “platy” (flat or platelike, as seen in the beak of a platypus). Platysmal descent results in blunting of the neck angle and loss of neck firmness. Ultimately, platysmal laxity can cause the visible vertical neck banding of advanced age.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


