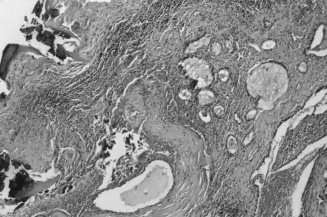
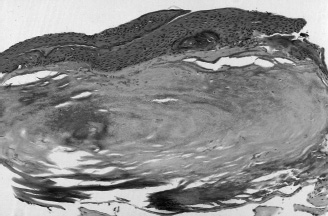
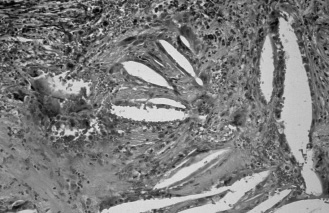
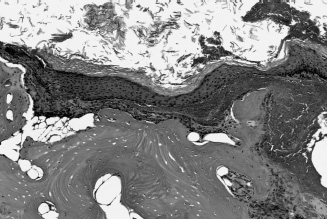
15 Middle ear and temporal bone pathology related to chronic ear disease includes infectious and inflammatory conditions, as well as complications secondary to chronic ear disease. The latter includes intratemporal complications (e.g., mastoiditis, petrositis, labyrinthitis) and in-tracranial complications. Rarely, neoplastic proliferations have been linked to long-standing chronic otitis media. This section discusses the pathological conditions related to the more common issues in chronic ear disease. ■ Infectious Conditions Otitis Media Otitis media is either an acute or a chronic infectious disease of the middle ear space. Otitis media is predominantly but not exclusively a childhood disease. The most common microorganisms implicated in disease of the middle ear are Streptococcus pneumoniae and Haemophilus influenzae. Uncommonly, otitis media may be caused by tuberculosis2; syphilis3; fungi, including Candida, Mucor, Cryptococcus, and Aspergillus4; and actinomycosis.5 The setting for some of these infections, particularly myocoses, is in patients who are diabetic or debilitated.4 In patients infected with human immunodeficiency virus (HIV) or who suffer from acquired immunodeficiency syndrome (AIDS), Pneumocystis carinii may seed from pulmonary lesions to the middle ear and temporal bone.6 Otoscopic examination reveals a hyperemic, opaque, bulging tympanic membrane with limited mobility; purulent otorrhea may be present. Bilateral involvement is not uncommon. The middle ear infection is felt to result from infection via the eustachian tube at the time of or following a pharyngitis (bacterial or viral). In general, otitis media is managed medically. However, at times tissue is removed for histopathologic examination. The pathological alterations are generally straightforward, but secondary changes such as glandular metaplasia of the surface epithelium, the result of chronic infection, may occur that might be confused with a true gland-forming neoplasm. Pathology There are no specific macroscopic features of otitis media. The tissue specimens usually are received as multiple small fragments of soft to rubbery granulation-appearing tissue. If tympanosclerosis is present, then the tissues may be firm to hard, consisting of calcific debris. In general, all of the tissue fragments should be processed for histologic examination. The histology of otitis media varies and depends on the disease state.7, 8 The histologic changes in chronic otitis media include a variable amount of chronic inflammatory cells consisting of lymphocytes, histiocytes, plasma cells, and eosinophils. Multinucleated giant cells and foamy histiocytes may be present. The middle ear low cuboidal epithelium may or may not be seen. However, glandular metaplasia, a response of the middle ear epithelium to the infectious process, may be present (Fig. 15–1)The glands tend to be more common in nonsuppurative otitis media than in suppurative otitis media. The metaplastic glands are unevenly distributed in the tissue specimens, are variable shaped, and are separated by abundant stromal tissue. The glands are lined by a columnar to cuboidal epithelium with or without cilia or goblet cell metaplasia. Glandular secretions may or may not be present, so that the glands may appear empty or contain varying secretions, including thin (serous) or thick (mucoid) fluid content. The identification of cilia is confirmatory of middle ear glandular metaplasia and is a feature not found in association with middle ear adenomas.1 Further, the haphazard arrangement of the glands in the background of changes of chronic otitis media should allow for differentiating metaplastic from neoplastic glands. Acute inflammatorycells may be superimposed bychronic otitis media. FIGURE 15-1 The histologic features of chronic otitis media include a background of chronic inflammation composed of lymphocytes with fibrosis and hemorrhage; scattered unevenly distributed metaplastic glands of variable size and shape containing thin (serous) fluid and separated by abundant stromal tissue are seen. Foci of calcification (tympanosclerosis) are present. To the lower right of the illustration the normal middle ear low cuboidal epithelium is seen. Acute otitis media is virtually never a surgical disease. The middle ear mucosa, also referred to as the mucoperiosteum, responds to infection with inflammation, hyperemia, polypoid thickening, and edema. The inflammatory infiltrate in acute otitis media is predominantly composed of polymorphonuclear leukocytes with a variable admixture of chronic inflammatory cells. Acute otitis media usually heals by resorption by the mucoperiosteum. However, localized destruction of the middle ear ossicles may occur. Further, granulation tissue may develop, resulting in scar formation. Fibrosing osteitis is seen in areas of bone destruction that may result in reactive sclerotic bone. In addition to the inflammatory cell infiltrate and glandular metaplasia, other histopathologic findings can be seen in association with chronic otitis media (or represent sequelae of chronic otitis media), including fibrosis, granulation tissue, tympanosclerosis, cholesterol granulomas, and reactive bone formation. Due to the presence of scar tissue, the middle ear ossicles may be destroyed (partial or total) or may become immobilized. Perforation of the tympanic membrane pars tensa may occur with resulting ingrowth of squamous epithelium, potentially leading to the development of cholesteatoma (see later discussion). Tympanosclerosis Tympanosclerosis represents dystrophic mineralization (calcification or ossification) of the tympanic membrane or middle ear that is associated with recurrent episodes of otitis media.8, 9 The incidence of tympanosclerosis in otitis media varies from 3 to 33%.10 Tympanosclerosis of the tympanic membrane can be seen in children following myringotomy and tube insertion. In this setting the tympanosclerotic foci may or may not be permanent. Tympanosclerosis of the middle ear typically affects older patients, represents irreversible accumulation of mineralized material, and is associated with conductive hearing loss.11, 12 Pathology On gross examination, tympanosclerotic foci may be localized or diffuse and appear as white nodules or plaques. Histologically, dense clumps of mineralized calcified or ossified material or debris can be seen within the stromal tissues or in the middle (connective tissue) aspect of the tympanic membrane (Fig. 15-2). Tympanosclerosis may cause scarring and ossicular fixation. Cholesterol Granulomas Cholesterol granuloma is a histologic designation describing the presence of a foreign body granulomatous response to cholesterol crystals derived from the rupture of red blood cells with breakdown of the lipid layer of the erythrocyte cell membrane. Cholesterol granulomas arise in the middle ear and mastoid in any condition in which there is hemorrhage combined with interference in drainage and ventilation of the middle ear space.13 Cholesterol granuloma of the middle ear may present as idiopathic hemotympanum; patients may also complain of hearing loss and tinnitus. The majority of cholesterol granulomas in the middle ear and temporal bone have an indolent biological behavior and cause no significant bone resorption. FIGURE 15-2 Tympanosclerosis in which prominent calcification (center) is adherent to the normal squamous epithelium of the tympanic membrane (top). In contrast to cholesterol granulomas of the middle ear and temporal bone, cholesterol granulomas of the petrous apex may behave aggressively, producing a tumorlike mass with expansion of the cyst and erosion/destruction of adjacent structures. Depending on the direction of expansion, apical cholesterol granulomas may invade into the cochlea, cerebellopontine angle, jugular foramen, cranial nerves V to XI, brain-stem, and cerebellum, producing life-threatening symp-toms.14 Involvement of the petrous apex is more likely to be associated with sensorineural hearing loss; additional signs and symptoms may include headaches, cranial nerve deficits, and bone erosion with involvement of the posterior or middle cranial fossa.14, 15 On axial computed tomography apical cholesterol granulomas appear as round to ovoid to irregular-appearing cysts with smooth margins and evidence of bone remodeling. Pathology The histology of cholesterol granulomas is the same irrespective of location and includes the presence of irregular-shaped, clear-appearing spaces surrounded by either or both histiocytes and multinucleated giant cells (foreign body granuloma) (Fig. 15–3). Cholesterol granulomas are not related to cholesteatomas but may occur in association with or independent of a chole-steatoma. FIGURE 15-3 Cholesterol granuloma appears as empty, irregularly shaped clefts or spaces surrounded by histiocytes and multinucleated giant cells. Fresh hemorrhage and hemo-siderin pigment are readily apparent. Cholesteatoma (Keratoma) Cholesteatoma is a pseudoneoplastic lesion of the middle ear characterized by the presence of stratified squamous epithelium that forms a saclike accumulation of keratin within the middle ear space (akin to an epidermal inclusion cyst). Despite their invasive growth, cholesteatomas are not considered to be true neoplasms. The term cholesteatoma is a misnomer in that it is not a neoplasm nor does it contain cholesterol.16 Perhaps the designation of keratoma would be more accurate, but the term cholesteatoma is entrenched in the literature. In the middle ear and inner ear, cholesteato-mas take three forms: acquired cholesteatoma, congenital cholesteatoma, and cholesteatoma of the petrous apex. Depending on the site of origin in the tympanic membrane, each of these cholesteatomas may be subdivided into pars flaccida (Shrapnell’s membrane) and pars tensa cholesteatomas. Acquired Cholesteatoma Acquired cholesteatomas are the most common type of cholesteatoma. They tend to be more common in men than in women and occur in older children and young adults. Acquired cholesteatoma is derived from entry of external ear canal epidermis into the middle ear. This may occur in one of several ways: via perforation of the tympanic membrane, following localized retraction of the tympanic membrane with epithelial invagination or ingrowth of a band of stratified squamous epithelium into the middle ear, via entrapment of squamous epithelium following surgery or trauma, or via squamous metaplasia of the middle ear mucosa.17, 18 The upper posterior part of the middle ear space is the most common site of acquired cholesteatomas. Initially, cholesteatomas may remain clinically silent until extensive invasion of the middle ear space and mastoid occurs. Symptoms include hearing loss, malodorous discharge, and pain and may be associated with a polyp arising in the attic of the middle ear or perforation of the tympanic membrane. Otoscopic examination may reveal the presence of white debris within the middle ear, which is considered diagnostic. Congenital Cholesteatoma Congenital cholesteatoma is a cholesteatoma of the middle ear that exists in the presence of an intact tympanic membrane, presumably occurring in the absence of chronic otitis media, that may result in perforation or retraction of the tympanic membrane. Congenital cholesteatomas are found in infants and young children. Small colonies of epidermoid cells referred to as epidermoid formations are found on the lateral anterosuperior surface of the middle ear in temporal bones after 15 weeks’ gestation.17 During the first postpartum year the epidermoid colonies disappear; however, if the epidermoid cells do not disappear but continue to grow, they will become a congenital cholesteatoma. The latter have also been referred to as epidermoid cysts.18 In the majority of cases congenital cholesteatomas are found in the anterosuperior part of the middle ear. In early lesions there are no symptoms, and they are discovered by otoscopic examination. In later lesions the signs and symptoms may be the same as acquired cholesteatoma. Cholesteatoma of the Petrous Apex Cholesteatoma of the petrous apex is an epidermoid cyst of this location and bears no relation to cholesteatoma of the middle ear. It is likely of congenital origin, but no cell rests have been discovered that may explain the origin of these lesions. Symptoms usually relate to involvement of the seventh and eighth cranial nerves in the cerebellopontine angle.19 Pathology Cholesteatomas appear as cystic, white to pearlymasses of varying size containing creamy or waxy granular material. The histologic diagnosis of cholesteatoma is made in the presence of a stratified keratinizing squamous epithelium, subepithelial fibroconnective or granulation tissue, and keratin debris (Fig. 15–4). The essential diagnostic feature is the keratinizing squamous epithelium; the presence of keratin debris alone is not diagnostic of a cholesteatoma. The keratinizing squamous epithelium is cytologically bland and shows cellular maturation without evidence of dysplasia. In spite of its benign histology, cholesteatomas are invasive and have widespread destructive capabilities. The destructive properties of cholesteatomas result from a combination of interrelated reasons, including mass effect with pressure erosion of surrounding structures from the cholesteatoma; the production of collagenase, which has osteodestructive capabilities by its resorption of bony structures; and bone resorption.20 Collagenase is produced by both the squamous epithelial and the fibrous tissue components of the cholesteatoma. This local aggressive behavior is the result of the continuing accumulation of the cholesteatomatous material with progressive erosion of surrounding structures. Depending on the location and extent of the cholestea-toma, erosion mayinclude the lateral wall of the attic, the middle ear ossicles, the tegmental bone over the attic and antrum, and the mastoid cortex.17 Less frequent progression includes erosion of the lateral sinus and jugular bulb, the vestibular and cochlear capsules, the fallopian canal, the dura of the middle and posterior cranial fossa, the semicircular canals, and the facial nerve.17 Sequelae of such erosions may include semicircular canal fistulas, exposed tympanic facial nerve, or brain herniation through the tegmen. FIGURE 15-4 The histologic diagnosis of cholesteatoma is based on the presence of finding keratinizing squamous epithelium within the middle ear space. The histologic diagnosis of cholesteatomas is relatively straightforward in the presence of keratinizing squamous epithelium. In contrast to cholesteatomas, squamous cell carcinoma shows dysplastic or overtly malignant cytological features, with a prominent desmoplastic stromal response to its infiltrative growth. Cholesteatomas do not transform into squamous cell carcinomas. In an attempt to determine whether cholesteatomas were low-grade squamous carcinomas, Desloge et al21 performed DNA analysis on human cholesteatomas to determine whether ploidy abnormalities were present. In 10 cases with interpretable data, nine were euploid, and one was aneuploid. These authors concluded that due to a lack of overt genetic instability, cholesteatomas could not be considered to be malignant neoplasms. Cholesterol granuloma is not synonymous with cholesteatoma. These entities are distinctly different pathological entities and should not be confused with one another.16 Keratosis obturans results when the normal self-cleaning mechanism of keratin maturation and lateral extrusion from the external auditory canal is defective. This causes accumulation of keratin debris deep within the bony aspect of an excavated external auditory canal. The etiology of keratosis obturans remains unclear. Keratosis obturans occurs most commonly in the first two decades of life, and symptoms generally relate to conductive hearing loss due to the keratin plug. Pain or bleeding is not an uncommon finding. The keratin debris may exert pressure effects on the bony canal wall, resulting in widening of the external auditory canal, bone remodeling, and inflamed epithelium. The histologic appearance is that of tightly packed keratin squames in a lamellar pattern. The treatment for keratosis obturans is debridement of the keratin plug.
Temporal Bone Pathology Related to Chronic Ear Disease
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


