and Charles P. Molumi2
(1)
University of Papua New Guinea and Port Moresby General Hospital, Boroko, National Capital District, Papua New Guinea
(2)
Port Moresby General Hospital, Boroko, National Capital District, Papua New Guinea
9.1 Subtotal Petrosectomy for Middle Ear Carcinoma with Facial Palsy

Fig. 9.1
Postauricular incision used for elevation of anterior musculoperiosteal flap and identification of the facial nerve is marked out. The incision is extended into the neck for exposure of the great vessels and cranial nerves. The upper limb of the incision is marked out for temporalis muscle mobilization if needed after the procedure
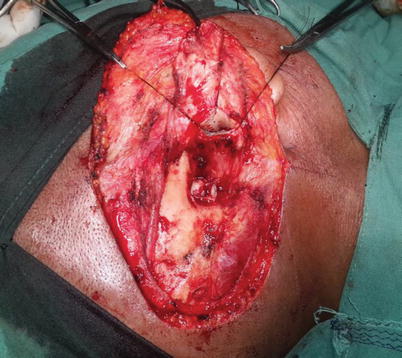
Fig. 9.2
Anteriorly based mastoid musculoperiosteal flap is raised and left attached to the catalagenous canal to be used later for obliteration of the mastoid cavity
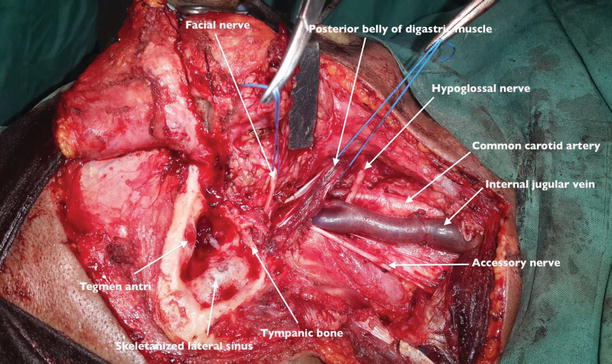
Fig. 9.3
Neck dissection is done and the facial nerve identified. The facial nerve is dissected into the parotid gland postauricularly and up to the point of second division. The sternocleidomastoid muscle is retracted posteriorly and common carotid artery, internal jugular vein and vagus nerve identified. Cranial nerves XI and XII are also identified. Total parotidectomy is done. The tympanic segment of the facial nerve is removed as it is involved by the tumor. Radical mastoidectomy is done
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


