(1)
Alo Eye Care, Kolkata, India
Keywords
Anterior lamellar reconstructionAdvancement flapsSkin graftsPosterior lamellar reconstruction16.1 Anterior Lamellar Reconstruction
16.1.1 Technique of Primary Closure
16.1.1.1 Indications
Small circular or elliptical skin defects in the upper or lower lid not involving the lid margin.
16.1.1.2 Technique
Small skin defects in the lower lid are repaired vertically, this helps in following the skin tension lines, thus preventing any postoperative contracture induced ectropion. For significant defects in which undue tension or stretching results in the apposition line, flap mobilization is a better option.
For skin defects of the upper lid not involving the lid margin, apposition may be attempted in a horizontal oval manner. This will fall within the superior lid folds, thus minimizing visible scarring.
16.1.1.3 Other Options/Variations
A circular skin defect may be made into a vertical oval for the upper lid and a horizontal oval for the lower lid. This prevents dog-ear formation at the two ends.
Eyelid skin incisions heal very well, rarely resulting in a visibly unacceptable scar. Any scar may be softened by massage with a topical steroid ointment. Prominent scars may be managed with a simple Z-plasty in the long run.
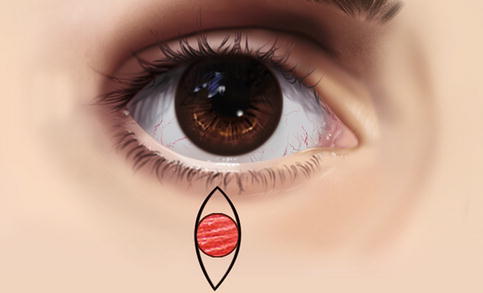
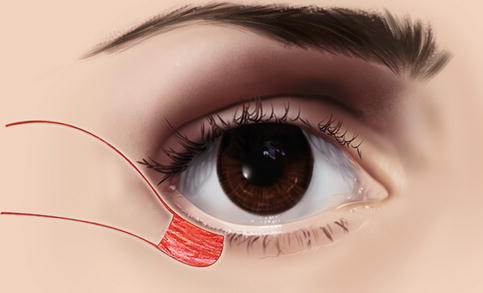
Fig. 16.1
Technique of repair of small circular lower periorbital skin defects (direct closure). A small circular skin defect

Fig. 16.2
Technique of repair of small circular lower periorbital skin defects (direct closure). The skin surrounding the defect is excised so that the defect takes the shape of a vertical oval
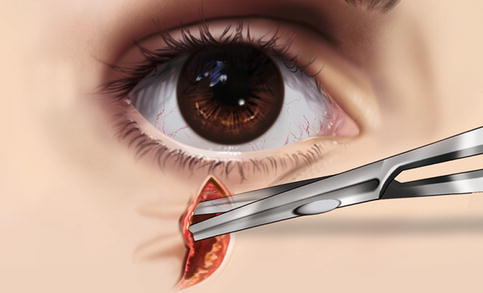
Fig. 16.3
Technique of repair of small circular lower periorbital skin defects (direct closure). Undermining is done in a submuscular plane around the defect to bring the cut margins into apposition
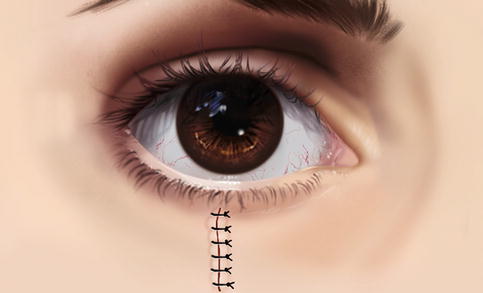
Fig. 16.4
Technique of repair of small circular lower periorbital skin defects (direct closure). The defect is repaired in a single layer with interrupted sutures
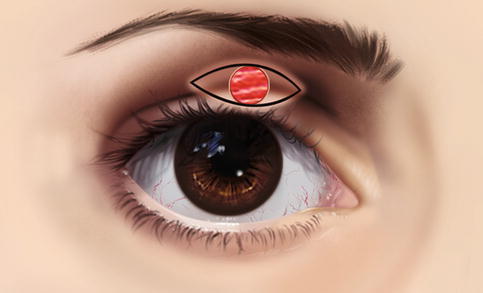
Fig. 16.5
Direct closure of small circular upper periorbital skin defects. A small circular skin defect
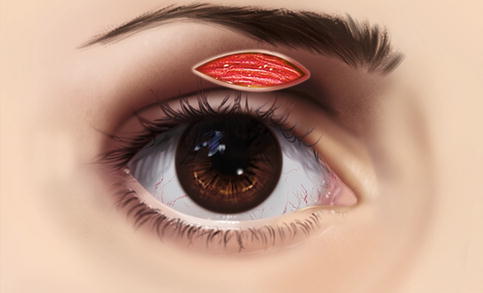
Fig. 16.6
Direct closure of small circular upper periorbital skin defects. The skin surrounding the defect is excised so that the skin defect takes the shape of a horizontal oval
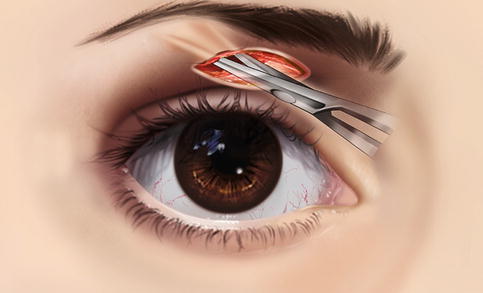
Fig. 16.7
Direct closure of small circular upper periorbital skin defects. Undermining is done in a submuscular plane around the defect to bring the cut margins into apposition

Fig. 16.8
Direct closure of small circular upper periorbital skin defects. The defect is repaired in a single layer with interrupted sutures

Fig. 16.9
Direct closure of small circular lower periorbital skin defects. A triangular incision is marked below the lower lid skin defect

Fig. 16.10
Direct closure of small circular lower periorbital skin defects. The tissue triangle is dissected in a submuscular plane, with care taken to leave a small stump from the underlying bed

Fig. 16.11
Direct closure of small circular lower periorbital skin defects. The skin flap is mobilized upward to fill the tissue defect and is closed in a Y
16.1.2 Technique of Skin Advancement Flaps
16.1.2.1 Indications
If the skin defect appears too large for direct apposition, mobilization of a skin flap and advancement from the surrounding skin should be planned.
This approach provides better cosmesis in maintaining skin color, as well as a greater chance of acceptance with respect to free skin grafts.
16.1.2.2 Technique
The most lax skin surrounding the skin defect is identified, and an advancement flap is planned.
Where long advancement flap mobilization requires significant undermining of tissue, a rotational flap should be planned.
In cases in which laxity is present on both sides of the skin defect, a double-advancement flap from both sides should be planned.
16.1.2.3 Other Options/Variations
Rotational flaps may be mobilized in the form of a simple rotation or may be bilobed, rhomboid, or Dufourmentel flaps.
Advancement flaps may be monopedicle or bipedicle.