Technique for the Surgical Excision of Carotid Body Tumors
James L. Netterville
INTRODUCTION
The carotid body tumor (CBT) is the most common paraganglioma arising within the head and neck region. Paragangliomas are tumors that arise from the branchiomeric paraganglia, which are distributed from the skull base down to the aortic arch. These neoplasms may also arise from paraganglia of the middle ear (tympanic paraganglioma), the jugular bulb, the vagus nerve at the skull base or in the neck, and the sympathetic trunk. Less frequently, these tumors may arise in the larynx, thyroid gland, and intrathoracic region around the aortic arch.
Our institution and others have established in the literature that resection of these tumors is not only technically feasible but can be done on a routine basis with low morbidity. Cranial nerve injury still remains the most common sequela of surgical treatment of CBTs. First bite syndrome, described as intense preauricular pain (periparotid) with initial bites of each meal, is also seen frequently after the resection of these tumors. Baroreceptor failure, which can rarely occur in a transient fashion after unilateral resection, can be a severe and debilitating sequela after bilateral tumor resection, related to the loss of carotid sinus feedback.
The management of CBTs has evolved over the last several decades. Significant changes in the evaluation and treatment include (1) decreased use of diagnostic angiography secondary to improvements in computed tomography (CT) and magnetic resonance imaging (MRI); (2) increased incidence in nonoperative observation in asymptomatic older patients; (3) greater emphasis on preservation of the cranial nerves during resection; and (4) limited targeted use of preoperative embolization for massive complex CBT.
HISTORY
Patients commonly present within one of three subgroups: (1) an asymptomatic mass in the neck; (2) an incidental finding discovered on a CT or MRI scan, performed for evaluation of a separate problem; and (3) as members of family with inherited paraganglioma syndrome. In the past, the majority of these patients presented with an asymptomatic mass in the neck. However, with the significant increase in the use of imaging of the head and neck over the last two decades, more than half of the patients now present with a less obvious tumor incidentally noted on CT or MRI. A CBT <2.5 cm is difficult to palpate unless it presents in a very thin individual. If one is diligent in evaluating the history of patients with CBTs, other family members are commonly discovered with paragangliomas. Although it is commonly cited that <10% of patients have familial tumors, I have noted that 32% of the CBT patients in my series have familial paraganglioma syndrome.
The vast majority of these patients are asymptomatic with no deficits in adjacent cranial nerve function. A small number of patients with tumors >5 cm present with complaints of weak voice and dysphagia secondary to deficits in function of the vagus and hypoglossal nerves. In patients with CBT presenting with preoperative cranial nerve deficits one must rule out an occult vagal or jugular paraganglioma which is far more likely to cause nerve damage.
PHYSICAL EXAMINATION
During the physical examination for evaluation of a potential CBT, the surgeon should define the characteristics of the tumor, the function of the adjacent cranial nerves, examine the neck for the rare potential of metastatic lymph nodes and finally look for evidence of other head and neck paragangliomas.
Initially the neck is palpated to assess the size and location of the tumor and to discover other distinct masses. Classic teaching notes that one can move the CBT back and forth in the horizontal plane, but it has very little mobility to up and down pressure, resulting in little movement in the vertical plane. This finding is often very subtle and not a reliable indication to differentiate the CBT from other masses in the neck. Often one can feel the pulsation from the tumor, but this can also occur with metastatic nodes lying adjacent to the carotid artery. The contralateral neck is also carefully examined to ensure that other occult tumors are not overlooked.
Cranial nerves VII, IX, X, XI, and XII and the sympathetic trunk are evaluated for any deficits in function. If significant dysfunction of the cranial nerves is noted, it is often an indication of an occult vagal or jugular paraganglioma. A careful examination of the eyes must be performed to rule out Horner’s syndrome, which would indicate a primary tumor of the sympathetic trunk. One must also undertake a complete examination of the external auditory canal, the tympanic membrane, and the middle ear to rule out occult tympanic, jugular, or vagal tumors.
INDICATIONS
1. A resectable CBT in a young healthy patient
2. A small resectable contralateral CBT with multiple tumors putting the ipsilateral vagal and hypoglossal nerves at risk
3. CBT with suspected or proven malignant growth
4. Significant cervical mass effect in the otherwise asymptomatic patient
5. Patient preference with obvious tumor show in a thin neck
CONTRAINDICATIONS
1. An asymptomatic, slow-growing tumor in an older patient. This age cutoff is quite relative depending on the patient’s overall health and performance status.
2. Previous contralateral loss of vagal and or hypoglossal function
3. Patient preference in a stable or very slowly enlarging tumor
PREOPERATIVE PLANNING
With improvement in the quality of MRI, CT, and CT angiography, the need for preoperative arteriogram is now limited to the few larger tumors that undergo preoperative embolization. The most frequently used initial form of imaging to study the CBT is MRI. MRI/magnetic resonance angiography (MRA) has been shown to be very effective in identifying and evaluating paragangliomas of the head and neck. The ability of MRI/MRA to identify local recurrence as well as new primary lesions makes it the preferred imaging modality both in initial evaluation and for long-term follow-up.
It is rare for a CBT to present as a secreting tumor, with only 3% exhibiting neuroendocrine activity producing vasoactive amines (i.e., catecholamines and dopamine). However, most patients undergo a 24-hour urine evaluation for catecholamine secretion to rule out a vasoactive tumor.
Although many articles extol the benefits of preoperative embolization, it is a very invasive, expensive procedure that is often performed under monitored anesthesia. Avoiding the use of embolization for smaller tumors significantly reduces the length of hospital stay by 1 to 2 days, thereby reducing costs. For an experienced surgical team, it adds little benefit in tumors <5 cm.
Preoperative counseling is recommended for patients to better understand their postoperative clinical course. A thorough discussion is held with the patient and the family to explain baroreflex failure, first bite syndrome, the potential for cranial nerve deficits, and the rare chance of vascular complications. If tumor banking services are available, it is recommended to sign up the patients to participate in this valuable data collection process that will allow for further molecular and genetic evaluation. Finally a preoperative consultation is obtained with the vascular surgery team to be on standby to perform resection of the carotid and reconstruction as needed.
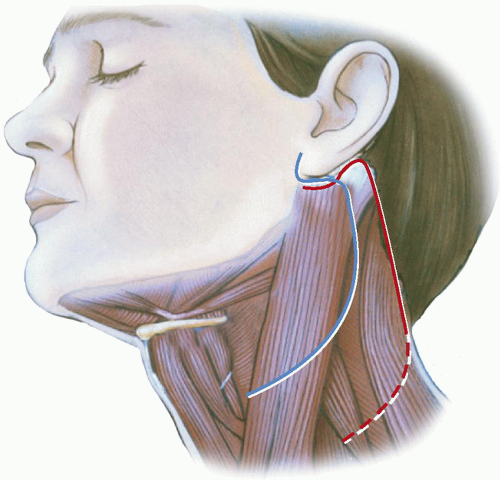 FIGURE 11.1 A central neck incision is outlined that may extend in the preauricular crease as needed to gain further access to the parapharyngeal space. In younger females, an extended hairline incision will give good exposure as well. Each incision must provide access to the carotid artery above and below the tumor dissection. |
SURGICAL TECHNIQUE
The major emphasis of this surgical procedure is neural preservation. Often during discussions on this topic, the emphasis is placed on the technical dissection of the carotid artery, with little attention paid to the cranial nerves. The main point to remember is that the carotid artery can be successfully grafted; however, significant injury to the vagus and hypoglossal nerves results in lifelong functional deficits in speech and swallowing. Early mobilization of these nerves away from the surface of the tumor, along with control of intraoperative bleeding, will prevent the vast majority of injuries that occur to these nerves. Although nerve monitoring of vagal function is gaining in popularity for tumors requiring dissection of the vagus and recurrent laryngeal nerves, it is rarely needed for the primary CBTs with no previous surgical dissection. It can be helpful in the dissection of recurrent tumors or those rare CBTs that have significant superior extension compressing the nerves as they exit the skull base.
A transcervical incision is placed in a cervical crease line as seen in Figure 11.1




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
