Purpose
To compare the results of tear film and lacrimal drainage system tests between anophthalmic socket and normal eye and assess discharge characteristics and frequency of prosthesis removal (questionnaire), eyelid function, and meibomian glad dysfunction (MGD).
Design
Prospective masked case control.
Methods
Subjects (≥6 years and ≥6 months of wearing prosthesis) with unilateral acquired anophthalmic socket discharge were included. Excluded was ocular adnexal abnormality of any reason and incomplete tests. The subjective questionnaire was completed. Blinking rate, lagophthalmos, eyelid laxity, MGD, Schirmer test, tear meniscus height, and dye disappearance test were assessed by a masked examiner. Another masked examiner performed an irrigation test 1 week later and interpreted the scintigraphy images at the end of the study.
Results
Included were 50 subjects (mean age: 31.3 years, mean prosthesis wear: 96.1 months). Discharge was frequent or very frequent in 85%, mucoid or mucopurulent in 90%, and moderate to severe in 86% of the subjects. MGD in 58%, lagophthalmos in 80%, and eyelid laxity in 46% were observed. Anophthalmic socket sides showed a significantly lower tear production and higher tear drainage obstruction. Subjects with frequent prosthesis removal had a significantly ( P = .02) greater lagophthalmos and blinking rate ( P = .04). The blinking rate was also significantly greater in subjects with higher frequency of discharge ( P = .04).
Conclusion
Tear film impairment (aqueous and lipid) and lacrimal drainage obstruction should be considered in subjects with anophthalmic socket discharge. A significantly higher blinking rate and lagophthalmos were found in subjects with higher frequency of prosthesis removal.
Discharge is the second concern, after the health of the normal eye, affecting 93% of subjects with anophthalmic socket, which has a variety of characteristics. Jang and associates reported a significantly high rate of meibomian gland dysfunction (MGD) in the anophthalmic sockets. Severe dryness of the socket because of diminished tear production (impaired Schirmer test) may occur in up to 75% of anophthalmic sockets. Little data exists regarding tear film and lacrimal drainage system findings in the setting of an ocular prosthesis. Furthermore, unrecognized lacrimal drainage system obstruction in anophthalmic sockets has been reported to presumably cause chronic discharge and contracted socket in a case report.
In the absence of a structural cause for anophthalmic socket discharge (implant exposure and infection, conjunctival cyst and granuloma, peg, etc), the prosthesis itself (improper fitting, handling, hygiene, deposits, roughness of the surface) and/or ocular adnexa (change in the conjunctival epithelium, impaired eyelid functions, impaired tear production and lacrimal drainage system) may play a role in producing the discharge.
We sought to correlate ocular adnexal findings (eyelid laxity, lagophthalmos, blinking rate, meibomian glad function, tear production, and lacrimal drainage system patency) and prosthesis handling with the presence, frequency, and type of anophthalmic socket discharge.
Methods
This prospective masked case-control study was approved by the ethics committee of Iran University Eye Research Center (21471/124/01/92) and was in line with the tenets of the Declaration of Helsinki. Informed consent was obtained from all the subjects.
In a pilot study, Schirmer and irrigation tests were performed on both the anophthalmic socket side and normal eyes of 15 subjects to calculate the sample size of the study. Mean Schirmer test was 5.2 mm (SD = 1.3) on the anophthalmic socket and 11.5 (SD = 1.1) on the normal side. To find a 20% difference (α = 5%, power = 90%), the sample was 22 subjects (22 cases and 22 controls). Lacrimal drainage diagnostic probing and irrigation showed an obstruction (partial or complete at different levels) in 13.3% of the normal side and 66.7% of anophthalmic socket side. To find a 20% difference (α = 5%, power = 90%), the sample size was 34 subjects (34 cases and 34 controls). They were not included in the main study.
Subjects with anophthalmic socket discharge (≥6 years of age for feasibility of performing the tests) who were wearing a prosthesis for more than 6 months and were under periodic care of their ocularists were consecutively included between March 1, 2013 and February 1, 2014. Excluded were improper prosthesis (displaced, extruding or rotating on/rubbing the eyelids, large or small size, rough surface), socket complications (socket contraction, anophthalmic socket syndrome, pyogenic granuloma, inclusion cyst, presence of peg, implant exposure, infection), using any regular drops except for artificial tear, and any systemic disease, surgery, or trauma affecting the ocular adnexal structures. Subjects with symptoms of watery or dry eye on the normal side were also excluded.
A discharge characteristics questionnaire was completed by the subjects under supervision of the first examiner (R.Z.) on the first visit. After recording of the demographics, type of eye removal procedure, and time of prosthetic fitting, the blinking rate at rest, lagophthalmos, lower eyelid laxity, MGD, upper eyelid palpebral conjunctiva, Schirmer test, tear meniscus height, lacrimal sac regurgitation test, and 5-minute fluorescein dye disappearance test were assessed and a lacrimal scintigraphy was requested by the first masked examiner (first visit). The second masked examiner (M.B.K.) assessed the puncti and performed a diagnostic lacrimal probing and irrigation test 1 week later (second visit), when the scintigraphy image print-outs were filed by the secretary. The scintigraphy images were then interpreted by the second examiner without knowing the side of the anophthalmic socket at the end of the study.
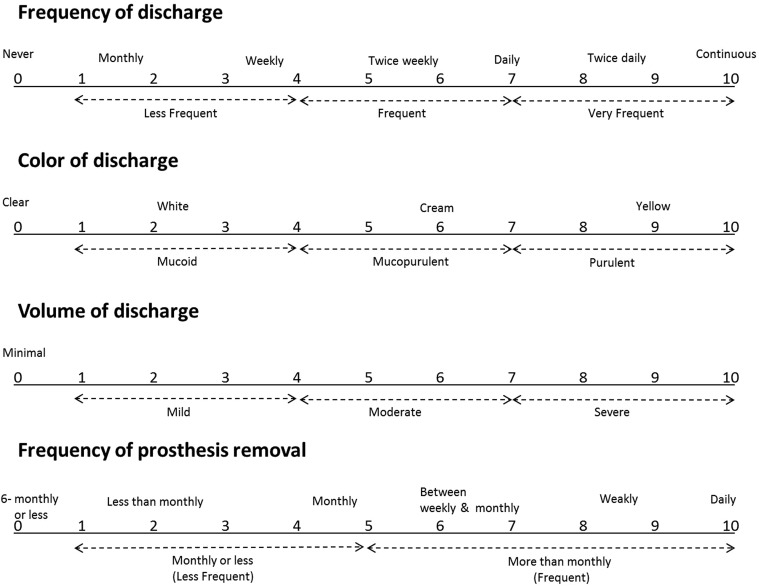
The questionnaire was a modification of Pine and associates’ questionnaire. Since our subjects reported that the “viscosity” question has the same answer as the “color” question and many participants did not answer the “viscosity” question, this was excluded from the questionnaire. The questionnaire was a visual analog scale with 0 (no or minimal) at the left and 10 (the most severe) at the right end of a line. For analysis, the analog scores for frequency, color, and volume were grouped into 3 levels, while the analog scores for frequency of prosthesis removal were grouped into 2 levels ( Figure ). Lower eyelid laxity, lagophthalmos, MGD, blinking rate at rest (number of blinks/minute), 5-minute Schirmer test, tear meniscus height based on slit-lamp examination, time and rate of positivity of fluorescein dye disappearance test (grade 0 and 1 as negative and grade 2 and 3 as positive), lacrimal sac regurgitation, and different types of anatomic lacrimal drainage system obstruction (punctal assessment, diagnostic probing, and irrigation test ) were recorded for the analysis. Scintigraphy results were classified as normal, presac, preduct, and intraduct obstruction based on Jabbour and associates’ criteria.
Since symptoms and eyelid/conjunctival signs of MGD could not be used for diagnosis of MGD in anophthalmic socket, plugged meibomian gland orifice involving ≥one-third of the lower eyelid was considered as MGD on the anophthalmic socket side in this study.
All the data were entered with SPSS (IBM SPSS Statistics for Windows, Version 19.0; IBM Corp, Armonk, New York, USA). Paired sample t test (comparing means between 2 sides), Wilcoxon signed rank test (comparing categorical data between 2 sides), independent sample t test (comparing means in categorical data with 2 options), 1-way analysis of variance with or without post hoc test (comparing means in categorical data with >2 options), and χ 2 test (comparing categorical data) were used for analysis. A P value of less than .05 was considered significant. All the variables were also assessed against duration of prosthetic wear, presence of eyelid laxity, MGD, and lagophthalmos in the anophthalmic socket sides.
Results
There were 66 consecutively recruited subjects with acquired unilateral anophthalmic socket, of whom 16 subjects were excluded because of socket complications (7), ocular adnexal trauma or surgery (4), incomplete visits (3), and being on eye drops (2). Included (50) were 28 female and 22 male subjects with a mean age of 31.3 (SD =16.8, range = 7–67) years. Mean time period of prosthetic wear was 96.1 (SD = 85.8, range = 6–408) months. Trauma (22), tumor (13), phthisis bulbi (13), panophthalmitis (1), and painful blind eye (1) were the reasons for enucleation (38), evisceration (8), and conjunctival flap (4) procedures. Conjunctival flap had been performed in subjects with traumatic autoenucleation who did not consent for further surgery.
All the subjects scored 1 or more for all the items in the questionnaire with regard to the discharge characteristics (frequency, color, volume) and prosthesis removal ( Table 1 ).
| Discharge | Frequency, n (%) |
|---|---|
| Color | |
| Purulent | 5 (10%) |
| Mucopurulent | 15 (30%) |
| Mucoid | 30 (60%) |
| Frequency | |
| Very frequent | 13 (26%) |
| Frequent | 30 (60%) |
| Less frequent | 7 (14%) |
| Volume | |
| Severe | 17 (34%) |
| Moderate | 26 (52%) |
| Mild | 7 (14%) |
| Frequency of prosthesis removal | |
| Frequent | 30 (60%) |
| Less frequent | 20 (40%) |
Conjunctival papillary reaction in all and some giant papillae in 3 subjects was observed on slit-lamp examination. MGD was present in 58% (29/50), different degrees of lagophthalmos (mean = 2.52 mm, SD =1.76, range = 1–8) in 80% (40/50), and lower eyelid laxity in 46% (23/50) of the subjects. Mean blinking rate was 17.8 blinks/minute (SD = 3.07, range = 11–25). No conjunctival papillary reaction, MGD, eyelid laxity, or lagophthalmos was observed on the normal side.
The lacrimal sac regurgitation test was negative in all subjects. The anophthalmic socket side, as compared to the normal side, showed a significantly lower Schirmer value and tear meniscus height and higher frequency of positive fluorescein dye disappearance test, anatomic lacrimal drainage system obstruction on irrigation, and physiological lacrimal drainage system obstruction on scintigraphy ( Table 2 ). The majority of lacrimal drainage system obstructions were incomplete ( Table 2 ) and in the upper parts (puncti, canaliculi, common canaliculus) of the lacrimal drainage system ( Table 3 ).
| Anophthalmic Socket (50) | Normal (50) | P Value | |
|---|---|---|---|
| FDDT | |||
| Mean (SD) [range], minutes | 11.4 (3.3) [5–15] | 6.9 (3.01) [5–15] | .001 |
| Positive | 44 (88%) | 17 (34%) | .001 |
| Negative | 6 (12%) | 33 (66%) | |
| Mean (SD) [range] TMH, mm | 0.1 (0.05) [0–0.3] | 0.2 (0.07) [0.1–0.4] | .001 |
| Mean (SD) [range] Schirmer test, mm | 5.4 (1.4) [3–8] | 11.6 (0.9) [10–14] | .001 |
| Scintigraphy | |||
| Normal | 14 (28%) | 39 (78%) | .001 |
| Partial obstruction | 13 (26%) | 6 (12%) | |
| Complete obstruction | 23 (46%) | 5 (10%) | |
| Irrigation | |||
| Normal | 23 (46%) | 42 (84%) | .001 |
| Partial obstruction | 24 (48%) | 7 (14%) | |
| Complete obstruction | 3 (6%) | 1 (2%) |
| Anophthalmic Socket (n = 50) | Normal (n = 50) | |
|---|---|---|
| Scintigraphy | ||
| Normal | 14 (28%) | 39 (78%) |
| Presac | 4 (8%) | 0 |
| Preduct | 25 (50%) | 8 (16%) |
| Intraduct | 7 (14%) | 3 (6%) |
| Irrigation test | ||
| Normal | 23 (46%) | 42 (84%) |
| P | 14 (28%) | 1 (2%) |
| C | 3 (6%) | 5 (10%) |
| CC | 1 (2%) | 1 (2%) |
| NLD | 3 (6%) | 1 (2%) |
| C + NLD | 2 (4%) | — |
| CC + NLD | 1 (2%) | — |
| P + NLD | 2 (4%) | — |
| P + C + NLD | 1 (2%) | — |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


