Purpose
To describe the cause and consequence of tear dysfunction–related corneal disease.
Design
Perspective on effects of tear dysfunction on the cornea.
Methods
Evidence is presented on the effects of tear dysfunction on corneal morphology, function, and health, as well as efficacy of therapies for tear dysfunction–related corneal disease.
Results
Tear dysfunction is a prevalent eye disease and the most frequent cause for superficial corneal epithelial disease that results in corneal barrier disruption, an irregular optical surface, light scattering, optical aberrations, and exposure and sensitization of pain-sensing nerve endings (nociceptors). Tear dysfunction–related corneal disease causes irritation and visual symptoms such as photophobia and blurred and fluctuating vision that may decrease quality of life. Dysfunction of 1 or more components of the lacrimal functional unit results in changes in tear composition, including elevated osmolarity and increased concentrations of matrix metalloproteinases, inflammatory cytokines, and chemokines. These tear compositional changes promote disruption of tight junctions, alter differentiation, and accelerate death of corneal epithelial cells.
Conclusions
Corneal epithelial disease resulting from tear dysfunction causes eye irritation and decreases visual function. Clinical and basic research has improved understanding of the pathogenesis of tear dysfunction–related corneal epithelial disease, as well as treatment outcomes.
The cornea is a truly unique optically clear tissue, devoid of blood vessels, that relies on tears to maintain a moist, smooth, and lubricated surface in the face of near-constant exposure to ambient environmental conditions during waking hours. Additionally, the tears provide myriad factors that protect the cornea from microbial infection and the sight-threatening effects of excessive inflammation or prolonged wound healing. To maintain corneal clarity and quality vision, humans have a complex and highly regulated system to produce and distribute tears.
Tear dysfunction is one of the most prevalent medical conditions, affecting tens of millions of patients worldwide. Tear dysfunction is a more encompassing term than dry eye for tear-associated disorders of the ocular surface and cornea because it encompasses changes in tear composition rather than tear volume. Tear dysfunction has long been recognized to cause corneal epithelial disease that can decrease visual performance and cause ocular irritation. Mechanisms responsible for these pathologic changes were poorly understood until evidence from recent clinical studies and animal models indicated that altered tear composition causes dysfunction, accelerated death, and detachment of the superficial epithelium, leading to an irregular corneal surface, an unstable tear layer, and hyperesthesia of the corneal nerve endings. These changes in the superficial cornea can significantly impact quality of life and productivity in patients suffering from tear dysfunction. I provide here my perspective on the function of tears on maintaining corneal health, the impact of tear dysfunction on the cornea, and consequences of tear dysfunction–related corneal disease on patient well-being based on published evidence and research I have performed over the past 25 years.
Vision Starts at the Tear Layer
The tear/corneal epithelial complex is the major light-refracting surface of the eye, accounting for approximately 65% of the optical power of the eye. A smooth and stable tear layer is essential for maintaining high-quality vision between blinks. Ultrastructural, biochemical, and functional studies show that the precorneal tear layer is a gel composed of soluble mucus secreted by the conjunctival goblet cells and fluid and proteins secreted by the lacrimal glands. This hydrophilic gel moves over the membrane mucins (glycocalyx) on the superficial corneal epithelial cells and serves as a medium to refresh the tear components and clear debris. The precorneal tear layer provides a smooth coating over the irregular microplicae on apical corneal epithelia cells. The normal tear film remains stable for the entire interblink interval, although the precorneal layer has been observed by optical coherence tomography (OCT) to gradually thin at a rate of 4 μm/minute because of evaporation and the pull of gravity toward the inferior meniscus. The precorneal tear layer is replenished from the reservoir of tears in the inferior tear meniscus by blinking. This meniscus contains 75% to 90% of the tear volume ( Figure 1 ) .

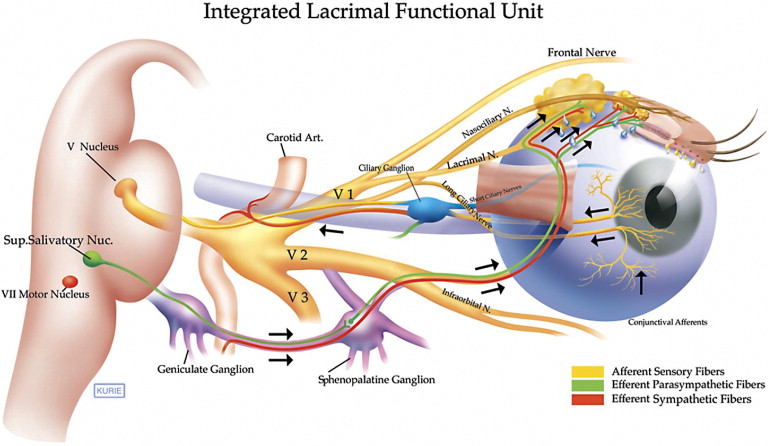
To maintain continuous unobstructed vision, the eye is open 92% of the time, with a blink rate of 15 times per minute. This renders the cornea the most exposed mucosal surface in the body. Thus, the corneal surface is presented with the challenge of resisting desiccation and maintaining a smooth optical surface during inter-blink intervals. It must also be capable of surviving environmental, occupational, and recreational desiccating stress. To maintain clarity, the cornea must be resistant to microbial invasion and be capable of initiating rapid, scar-free healing after wounding. Because the cornea lacks blood vessels to supply the antimicrobial defense and wound-healing factors necessary to combat these challenges, it depends on the tears to deliver them. Humans have highly complex tear-secreting apparatus that we have termed the Lacrimal Functional Unit (LFU), to maintain a stable precorneal tear film ( Figure 2 ) . The LFU consists of an afferent component of trigeminal nociceptors in the cornea and ocular surface that synapse in the brainstem with autonomic and motor efferent nerves, as well as higher-order sensory neurons. Autonomic nerve fibers, primarily cholinergic, have been found to innervate the meibomian glands, conjunctival goblet cells, and main and accessory lacrimal glands. Motor efferent fibers stimulate the orbicularis oculi muscle to initiate blinking to express lipid secretions from the meibomian glands, spread tears over the corneal surface, and direct them into the lacrimal puncta.
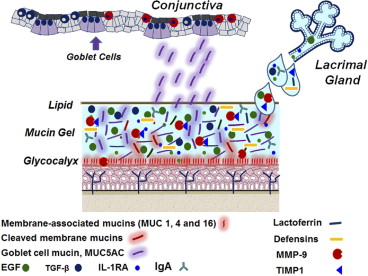
Tears contain a biochemically complex mixture of factors ( Table 1 ) that are produced by the lacrimal glands and ocular surface epithelium to lubricate, support, protect, and heal the cornea ( Figure 3 ) . Reflex tear secretion and blinking clear proteases and inflammatory mediators produced by the surface epithelium and resident immune cells that are capable of causing corneal epithelial disease through dilution and removal through the nasolacrimal duct system. Lipids secreted by the meibomian glands retard tear evaporation.
| Role | Component | References |
|---|---|---|
| Lubrication | MUC1, MUC4, MUC16, MUC5AC | |
| Wound healing | EGF, substance P, TGF-β | |
| Antimicrobial defense | Lactoferrin, lysosyme, defensins (α and β), IgA | |
| Anti-inflammatory | IL-1RA, TGF-β2 | , , |
| Protease inhibitors | TIMP1, SLPI | , |
Tear Dysfunction: A Major Clinical Problem
Tear dysfunction occurs when the lacrimal functional unit is no longer able to maintain a stable precorneal tear layer. It may develop from dysfunction or disease of 1 or more components of the lacrimal functional unit. Tear dysfunction is one of the most prevalent eye conditions. Epidemiologic studies performed worldwide on different populations and using a variety of diagnostic criteria have reported the prevalence to range from 2% to 14.4% depending on the study population and diagnostic criteria. This translates to a prevalence of tear dysfunction in between 6 and 43.2 million people in the United States. A number of risk factors for dry eye have been identified. Age is perhaps the biggest risk factor, with the prevalence increasing in both men and woman with every decade of life over the age of 40, with a greater prevalence in women than men at every age. Other risk factors identified include contact lenses, higher dietary consumption of n-6 to n-3 essential fatty acids, diabetes mellitus, cigarette smoking, prolonged video display viewing, and low-humidity environments. Patients with tear dysfunction typically report irritation symptoms including foreign body sensation, burning, and dryness, as well as vision-related symptoms such as photophobia and blurred and fluctuating vision. These symptoms may decrease quality of life in afflicted patients. In fact, the impact of tear dysfunction on quality of life was rated to be equivalent to unstable angina using utility assessments. In some cases, the consequences of tear dysfunction can be devastating and result in functional and occupational disability.
The majority of the symptoms of tear dysfunction result from corneal epithelial disease. Tear dysfunction has been recognized for over a century as the major cause of superficial corneal epithelial disease. It is now recognized that this epitheliopathy reduces corneal barrier function, causing an irregular optical surface, light scattering, optical aberrations, and exposure and sensitization of corneal nociceptors.
Tear Dysfunction: A Major Clinical Problem
Tear dysfunction occurs when the lacrimal functional unit is no longer able to maintain a stable precorneal tear layer. It may develop from dysfunction or disease of 1 or more components of the lacrimal functional unit. Tear dysfunction is one of the most prevalent eye conditions. Epidemiologic studies performed worldwide on different populations and using a variety of diagnostic criteria have reported the prevalence to range from 2% to 14.4% depending on the study population and diagnostic criteria. This translates to a prevalence of tear dysfunction in between 6 and 43.2 million people in the United States. A number of risk factors for dry eye have been identified. Age is perhaps the biggest risk factor, with the prevalence increasing in both men and woman with every decade of life over the age of 40, with a greater prevalence in women than men at every age. Other risk factors identified include contact lenses, higher dietary consumption of n-6 to n-3 essential fatty acids, diabetes mellitus, cigarette smoking, prolonged video display viewing, and low-humidity environments. Patients with tear dysfunction typically report irritation symptoms including foreign body sensation, burning, and dryness, as well as vision-related symptoms such as photophobia and blurred and fluctuating vision. These symptoms may decrease quality of life in afflicted patients. In fact, the impact of tear dysfunction on quality of life was rated to be equivalent to unstable angina using utility assessments. In some cases, the consequences of tear dysfunction can be devastating and result in functional and occupational disability.
The majority of the symptoms of tear dysfunction result from corneal epithelial disease. Tear dysfunction has been recognized for over a century as the major cause of superficial corneal epithelial disease. It is now recognized that this epitheliopathy reduces corneal barrier function, causing an irregular optical surface, light scattering, optical aberrations, and exposure and sensitization of corneal nociceptors.
Changes in Tear Composition and Corneal Epithelial Disease
Lacrimal gland disease, meibomian gland disease, and reduced tear clearance from ocular surface diseases such as conjunctivochalasis have been reported to alter tear composition ( Table 2 ). Conditions causing dysfunction of the lacrimal gland, such as Sjögren syndrome, result in significantly decreased concentrations of certain proteins and growth factors that are secreted by lacrimal acinar cells into tears, including lactoferrin and epidermal growth factor (EGF). Reduced tear EGF concentration was found to correlate with severity of corneal fluorescein staining in patients with tear dysfunction. Exposure of the corneal epithelium to increased osmolarity or to certain inflammatory/immune cytokines has been found to promote inflammation, abnormal differentiation, accelerated detachment, and programmed death (apoptosis) of the corneal epithelium ( Figure 4 ) . Elevated tear osmolarity, primarily attributed to increased Na+ ion concentration, is a common feature of tear dysfunction caused by lacrimal and meibomian gland disease. The mean osmolarity measured in tears—collected from the inferior meniscus in eyes with tear dysfunction—has been found to be about 20 to 40 mOsm/L greater than the normal tear film, ranging from 314 to 365 mOmol/L 29 ; however, osmolarity in areas of break-up of the precorneal tear layer has been calculated to be much higher and consistent with values of 560 mOsm/L measured in tear samples collected from the entire ocular surface of mice with experimentally induced dry eye. Exposure to a high-osmolality environment has been identified as a considerable stress to the corneal epithelium, resulting in activation of the mitogen-activated protein kinase (MAPK) and nuclear factor κB (NF-κB) stress signaling pathways in these cells ( Figure 4 ). These pathways initiate a cascade of events, including transcriptional activation of genes encoding inflammatory, matrix metalloproteinase (particularly MMP-9), and pro-apoptotic factors.
| Tear Component | Change | Reference |
|---|---|---|
| Sodium ion | ↑ osmolarity | |
| Growth factor | ↓ EGF | |
| Cytokine/chemokine | ↑ IFN-ϒ, IL-1, IL-6, IL-8, MIP-1α | |
| Protease | MMP-9 |
MMP-9 has been found to regulate physiological shedding of the corneal epithelium through lysis of the membrane-spanning tight junction protein occludin. In eyes with normal tear production, MMP-9 exists predominantly in a latent inactive form and the low levels of mature MMP-9 are bound to its physiological inhibitor, tissue inhibitor of matrix metalloproteinase 1 (TIMP1). MMP-9 activity increases in the closed eye during sleep when tear production and clearance decrease. A diurnal increase in MMP-9 expression was found to contribute to controlled extracellular cleavage of junctional complexes in the apical corneal epithelium in the Xenopus cornea and it may make a similar contribution to physiological turnover in the human cornea (Wiechmann AF, Pflugfelder SC, Howard E. IOVS 2011 ARVO Abstract 303). MMP-9 activity on the ocular surface increases in eyes with tear dysfunction because of increased production by stressed epithelial cells and infiltrating leukocytes, as well as increased activity of its physiological activators (eg, MMP-3) and reduced tear concentrations of TIMPs. Increased MMP-9 activity accelerates detachment of apical corneal epithelium, exposing less mature subapical epithelial cells and nociceptors, as shown in Figure 5 . Furthermore, loose epithelium, decreased surface lubrication, and friction from blinking exacerbates the problem and may promote development of filamentary keratitis. Disruption of the apical barrier can cause irritation and reduce visual performance, as discussed below. Pathways mediated by the stress kinase JNK2 were found to be primarily responsible for the MMP-mediated corneal barrier disruption in experimental dry eye. JNK2 has been reported to have a similar function in osmotically induced barrier disruption in the colonic epithelium.
In addition to the ocular surface epithelium, inflammatory mediators produced by inflammatory/immune cells that reside on the ocular surface or that are recruited to the conjunctival epithelium, particularly CD4+ T cells, were found to participate in the development of corneal epithelial disease in dry eye. Our group has found that exposure to desiccating stress recruits activated CD4+ T cells of the Th1 and Th17 lineages to the ocular surface. Interferon gamma (IFN-γ), the signature cytokine produced by Th1 cells, was found to induce apoptosis of the cornea and conjunctival epithelia, while interleukin 17 (IL-17) produced by Th17 cells stimulated production of MMPs 3 and 9 by the corneal epithelium. The corneal epithelium has been found to express receptors for both IFN-γ and IL-17.
Desiccation, osmotic stress, and the inflammatory cytokines IL-1 and IFN-γ can promote skin epidermal-like differentiation in the corneal epithelium with increased production of cornified envelope precursors that are absent or produced at low levels in unstressed corneal epithelial cells. Furthermore, exposure to high osmolarity activates intrinsic apoptotic pathways in corneal epithelial cells that can lead to accelerated turnover of the apical epithelium. Increased numbers of cornifying, dead, and detaching epithelial cells may be responsible for the increased number of opaque corneal epithelial cells that have been observed by confocal microscopy and metaplastic cells noted in conjunctival impression cytology of patients with tear dysfunction.
Clinical Consequences of Tear Dysfunction on the Superficial Cornea
The principal clinical manifestation of tear dysfunction–related superficial corneal epithelial disease is eye irritation. Typical symptoms consist of dryness, foreign body sensation, and burning. Patients often complain of exquisite sensitivity to wind or drafts from air conditioning vents. While the mechanisms responsible for these irritation symptoms are not fully understood, it appears they are attributable in large part to greater exposure of corneal nociceptors to environmental stimuli, as well as sensitization of these nerve endings by inflammatory mediators. Rosenthal and associates have proposed the term “corneal neuralgia” to describe the heightened corneal sensitivity associated with tear dysfunction. Transient receptor potential cation channel subfamily member 8 (TRPM8) ion channels in cold receptors in the corneal epithelium that increase firing as the temperature decreases from 34 to 24 C have been shown to regulate basal tear flow by the lacrimal gland. More rapid corneal cooling in eyes with tear dysfunction and accelerated tear break-up likely results in increased nerve firing that may be interpreted as eye discomfort. Studies evaluating corneal sensitivity in dry eye have reported conflicting results of either heightened or reduced sensitivity. Hyperesthesia has been observed in several studies using a gas esthesiometer, while studies testing mechanical sensitivity with a nylon monofilament have generally found reduced sensitivity to this mechanical stimulus. The conflicting findings of hyperesthesia or hypoesthesia in eyes with tear dysfunction may be attributed to the type of test stimulus applied or corneal nerve degeneration that may develop in eyes with long-standing tear dysfunction, particularly Sjögren syndrome.
Many patients with corneal epitheliopathy complain of photosensitivity that in some cases can be severe and disabling, forcing them to wear tinted glasses and avoid bright lights. This symptom may be attributed in part to light scattering from the irregular tear film and superficial corneal epithelium. Videokeratoscopic surface regularity indices have found greater surface irregularity in eyes with tear dysfunction that correlated with the severity of corneal fluorescein staining. Serial corneal topographic measurements taken of the open eye after a blink have observed a more rapid increase of corneal surface irregularity than eyes with normal tear function and the rate of change corresponded to the severity of corneal epithelial disease.
Corneal epithelial disease may also reduce optical performance. Many patients with tear dysfunction complain of fluctuating vision that may improve following instillation of artificial tears. Often patients with tear dysfunction have normal visual acuity measured by conventional methods; however, reduced visual performance has been found with more sophisticated measures of visual function. Patients with corneal epithelial disease were noted to have greater reduction in contrast sensitivity and low-contrast visual acuity than eyes with normal tear function. A number of studies have reported increased levels of higher-order aberrations, particularly coma, in eyes with tear dysfunction. These alterations in visual quality lead to a reduction in functional visual acuity.
Tear dysfunction can directly or indirectly increase the risk for developing microbial keratitis. Tear fluid contains factors that inhibit microbial attachment and invasion into the corneal epithelium. Corneal epitheliopathy from severe tear dysfunction has also been identified as a risk factor for microbial keratitis.
Eyes with reduced tear clearance associated with meibomian gland disease have been reported to have increased levels of tear EGF and VEGF that has been found to be associated with subepithelial fibrosis and peripheral vascularization.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


